Li Zhengteng, Liu Hongmei, Wang Min, Wang Xiankai, Pan Dongmei, Ma Aidong, Chen Yang
Department of Radiology, Jining No.1 People's Hospital, No. 6 Jiankang Road, Rencheng District, Jining, 272000, China.
Thyroid and Breast Surgery, Jining No.1 People's Hospital, No. 6 Jiankang Road, Rencheng District, Jining, 272000, China.
BMC Med Imaging. 2024 Jun 12;24(1):143. doi: 10.1186/s12880-024-01305-5.
This study developed and validated a nomogram utilizing clinical and multi-slice spiral computed tomography (MSCT) features for the preoperative prediction of Ki-67 expression in stage IA lung adenocarcinoma. Additionally, we assessed the predictive accuracy of Ki-67 expression levels, as determined by our model, in estimating the prognosis of stage IA lung adenocarcinoma.
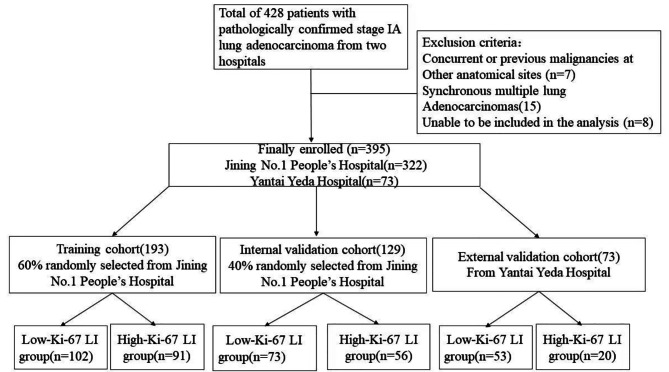
We retrospectively analyzed data from 395 patients with pathologically confirmed stage IA lung adenocarcinoma. A total of 322 patients were divided into training and internal validation groups at a 6:4 ratio, whereas the remaining 73 patients composed the external validation group. According to the pathological results, the patients were classified into high and low Ki-67 labeling index (LI) groups. Clinical and CT features were subjected to statistical analysis. The training group was used to construct a predictive model through logistic regression and to formulate a nomogram. The nomogram's predictive ability and goodness-of-fit were assessed. Internal and external validations were performed, and clinical utility was evaluated. Finally, the recurrence-free survival (RFS) rates were compared.
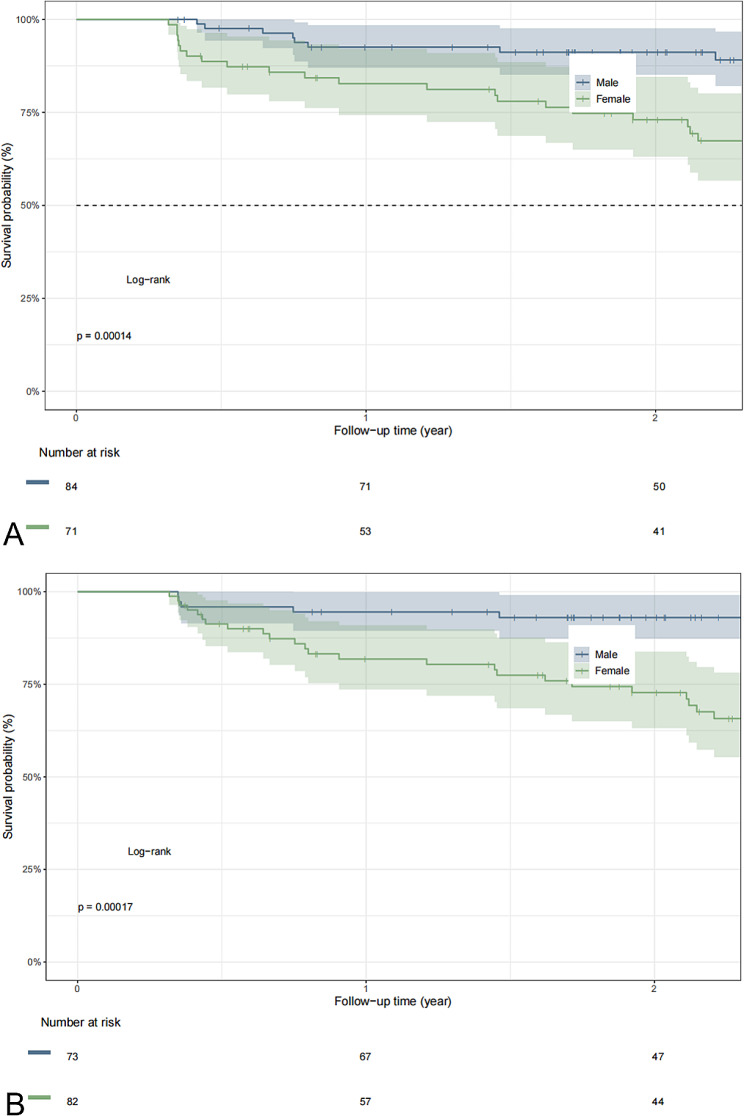
In the training group, sex, age, tumor density type, tumor-lung interface, lobulation, spiculation, pleural indentation, and maximum nodule diameter differed significantly between patients with high and low Ki-67 LI. Multivariate logistic regression analysis revealed that sex, tumor density, and maximum nodule diameter were significantly associated with high Ki-67 expression in stage IA lung adenocarcinoma. The calibration curves closely resembled the standard curves, indicating the excellent discrimination and accuracy of the model. Decision curve analysis revealed favorable clinical utility. Patients with a nomogram-predicted high Ki-67 LI exhibited worse RFS.
The nomogram utilizing clinical and CT features for the preoperative prediction of Ki-67 expression in stage IA lung adenocarcinoma demonstrated excellent performance, clinical utility, and prognostic significance, suggesting that this nomogram is a noninvasive personalized approach for the preoperative prediction of Ki-67 expression.
本研究开发并验证了一种列线图,该列线图利用临床和多层螺旋计算机断层扫描(MSCT)特征对ⅠA期肺腺癌患者术前Ki-67表达进行预测。此外,我们评估了通过我们的模型确定的Ki-67表达水平在估计ⅠA期肺腺癌预后方面的预测准确性。
我们回顾性分析了395例经病理确诊的ⅠA期肺腺癌患者的数据。总共322例患者按6:4的比例分为训练组和内部验证组,其余73例患者组成外部验证组。根据病理结果,将患者分为高、低Ki-67标记指数(LI)组。对临床和CT特征进行统计分析。训练组用于通过逻辑回归构建预测模型并制定列线图。评估列线图的预测能力和拟合优度。进行内部和外部验证,并评估临床实用性。最后,比较无复发生存(RFS)率。
在训练组中,高、低Ki-67 LI患者的性别、年龄、肿瘤密度类型、肿瘤-肺界面、分叶、毛刺征、胸膜凹陷及最大结节直径存在显著差异。多因素逻辑回归分析显示,性别、肿瘤密度和最大结节直径与ⅠA期肺腺癌高Ki-67表达显著相关。校准曲线与标准曲线高度相似,表明该模型具有出色的区分度和准确性。决策曲线分析显示出良好的临床实用性。列线图预测为高Ki-67 LI的患者RFS较差。
利用临床和CT特征对ⅠA期肺腺癌术前Ki-67表达进行预测的列线图表现出优异的性能、临床实用性和预后意义,表明该列线图是一种用于术前预测Ki-67表达的非侵入性个性化方法。