Department of Biomedical Sciences, University of Antwerp, Antwerp, Belgium.
Department of Neurology, Universitair Ziekenhuis Brussel (UZ Brussel), Brussels, Belgium.
Alzheimers Res Ther. 2024 Jun 14;16(1):128. doi: 10.1186/s13195-024-01491-y.
This study aimed to evaluate the potential clinical value of a new brain age prediction model as a single interpretable variable representing the condition of our brain. Among many clinical use cases, brain age could be a novel outcome measure to assess the preventive effect of life-style interventions.
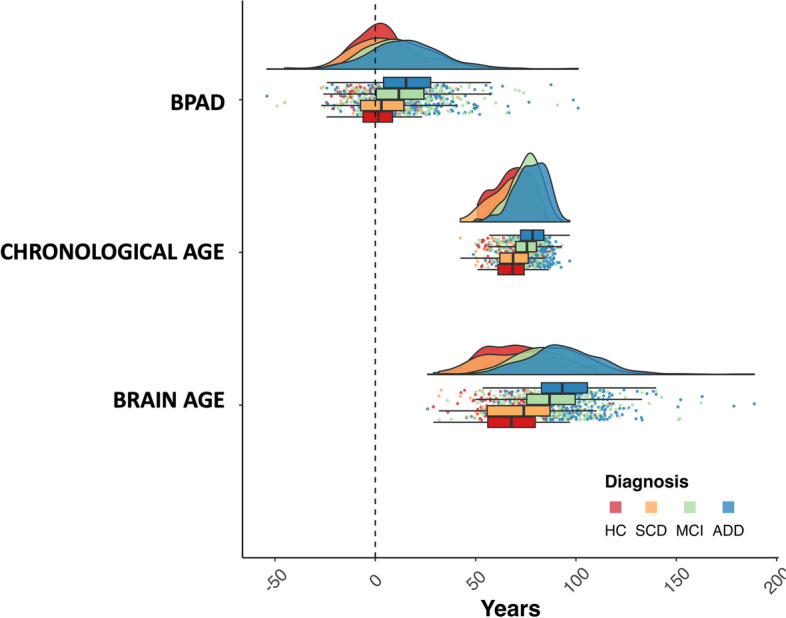
The REMEMBER study population (N = 742) consisted of cognitively healthy (HC,N = 91), subjective cognitive decline (SCD,N = 65), mild cognitive impairment (MCI,N = 319) and AD dementia (ADD,N = 267) subjects. Automated brain volumetry of global, cortical, and subcortical brain structures computed by the CE-labeled and FDA-cleared software icobrain dm (dementia) was retrospectively extracted from T1-weighted MRI sequences that were acquired during clinical routine at participating memory clinics from the Belgian Dementia Council. The volumetric features, along with sex, were combined into a weighted sum using a linear model, and were used to predict 'brain age' and 'brain predicted age difference' (BPAD = brain age-chronological age) for every subject.
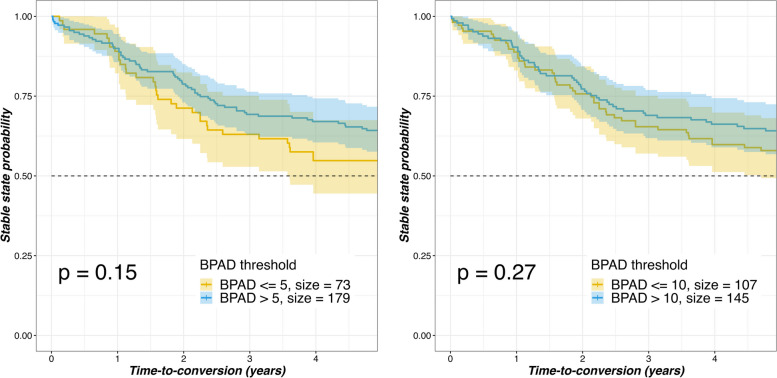
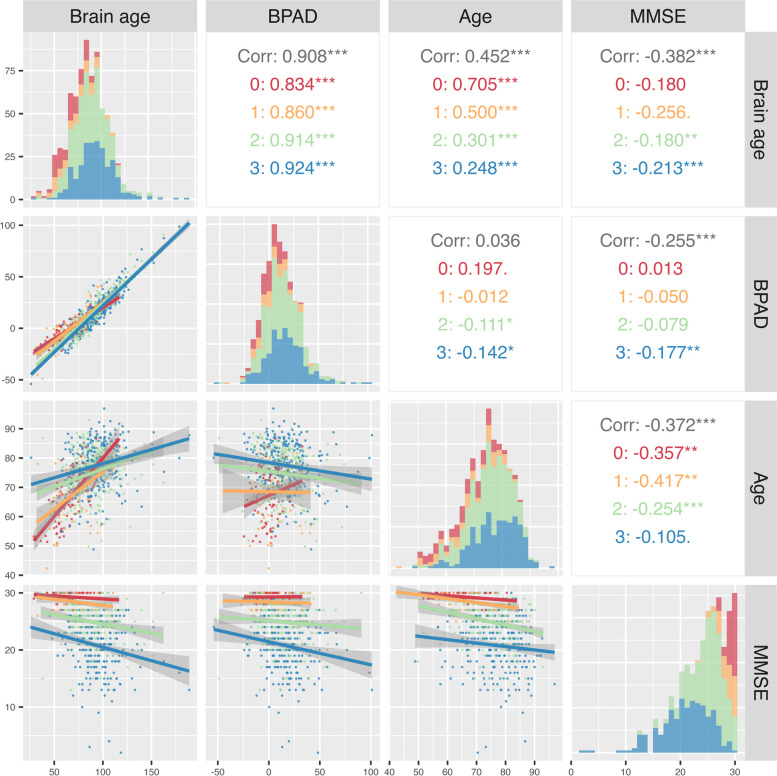
MCI and ADD patients showed an increased brain age compared to their chronological age. Overall, brain age outperformed BPAD and chronological age in terms of classification accuracy across the AD spectrum. There was a weak-to-moderate correlation between total MMSE score and both brain age (r = -0.38,p < .001) and BPAD (r = -0.26,p < .001). Noticeable trends, but no significant correlations, were found between BPAD and incidence of conversion from MCI to ADD, nor between BPAD and conversion time from MCI to ADD. BPAD was increased in heavy alcohol drinkers compared to non-/sporadic (p = .014) and moderate (p = .040) drinkers.
Brain age and associated BPAD have the potential to serve as indicators for, and to evaluate the impact of lifestyle modifications or interventions on, brain health.
本研究旨在评估一种新的大脑年龄预测模型的潜在临床价值,该模型可作为单一可解释变量来代表大脑状况。在许多临床应用案例中,大脑年龄可以作为一种新的结果测量指标,用于评估生活方式干预的预防效果。
REMEMBER 研究人群(N=742)包括认知健康(HC,N=91)、主观认知下降(SCD,N=65)、轻度认知障碍(MCI,N=319)和阿尔茨海默病痴呆(ADD,N=267)患者。从比利时痴呆症委员会参与记忆诊所的临床常规中获取的 T1 加权 MRI 序列中,使用 CE 标记和 FDA 批准的软件 icobrain dm(痴呆症)自动提取全脑、皮质和皮质下脑结构的容积特征,以及性别。使用线性模型将容积特征与性别相结合,形成一个加权和,用于预测每个患者的“大脑年龄”和“大脑预测年龄差”(BPAD=大脑年龄-实际年龄)。
与实际年龄相比,MCI 和 ADD 患者的大脑年龄增加。总体而言,在 AD 谱中,大脑年龄在分类准确性方面优于 BPAD 和实际年龄。总 MMSE 评分与大脑年龄(r=-0.38,p<0.001)和 BPAD(r=-0.26,p<0.001)之间存在弱至中度相关性。在从 MCI 向 ADD 转化的发生率方面,BPAD 与转化率之间存在明显趋势,但无显著相关性;在从 MCI 向 ADD 转化的时间方面,BPAD 与转化率之间也存在明显趋势,但无显著相关性。与非/偶发性(p=0.014)和中度(p=0.040)饮酒者相比,重度饮酒者的 BPAD 更高。
大脑年龄及其相关的 BPAD 有可能作为大脑健康的指标,并评估生活方式改变或干预对大脑健康的影响。