Department of Medical Ultrasonics, Affiliated Hospital of Jiangsu University, Zhenjiang, 212001, China.
Department of Obstetrics, Affiliated Hospital of Jiangsu University, Zhenjiang, 212001, China.
BMC Pregnancy Childbirth. 2024 Jun 15;24(1):431. doi: 10.1186/s12884-024-06562-4.
To evaluate the potential connections between marginal cord insertion during the first trimester and furcate cord insertion later in pregnancy.
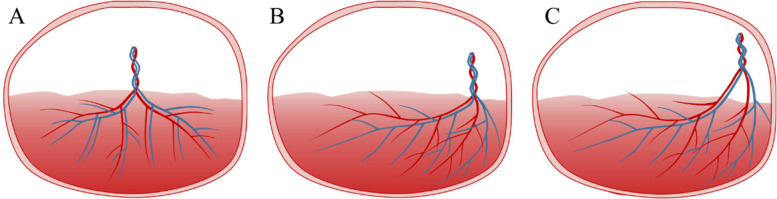
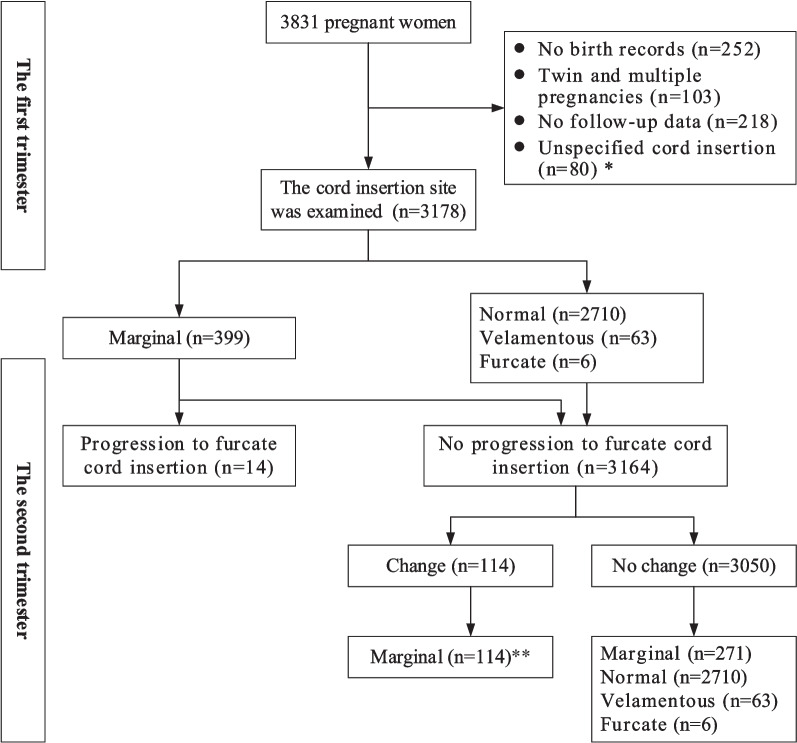
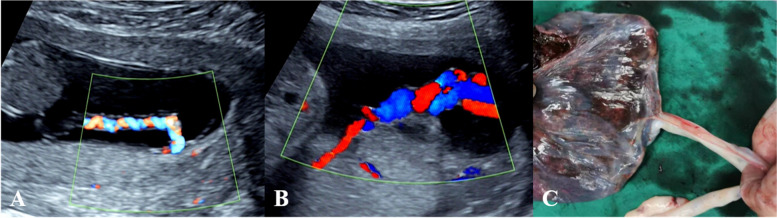
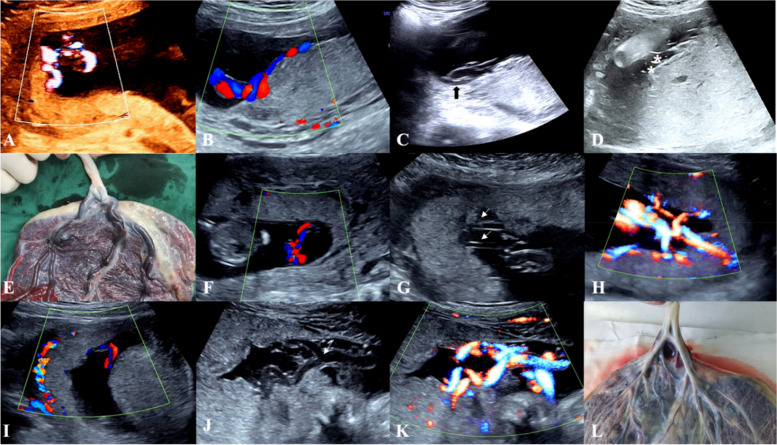
This is a prospective study of screening data on the cord insertion site in 3178 singleton pregnancies. The cord insertion site was examined in two stages. The first stage was screening for the cord insertion site between 10-13 weeks of gestation, the purpose is to determine the category of umbilical cord insertion. The second stage, performed at 22-28 weeks of gestation, was to follow up on the relationship between the cord insertion site and the placenta and to identify any changes in the category of umbilical cord insertion. This was performed to diagnose or exclude furcate cord insertion by identifying whether the umbilical cord trunk separated or branched before it reached the placenta. Factors influencing progression to furcate cord insertion and perinatal complications were assessed.
Fourteen cases (0.44%) with progression to furcate cord insertion, all of which showed marginal cord insertion on ultrasound in the first trimester (p < 0.001). without progression to furcate cord insertion, there were no changes in the category of umbilical cord insertion in 3050 cases (96.40%) compared to the early pregnancy. 114 cases (3.60%) with changes in the category of umbilical cord insertion that was not consistent with furcate cord insertion. A total of 14 cases progressed to furcate cord insertion, all showed the cord insertion site were in close proximity, and 11 (78.57%) cases showed a low insertion site (p < 0.001). Regarding the choice of mode of delivery, elective caesarean delivery was done in 8/14 (57.14%). The incidences of spontaneous vaginal delivery were 5/14 (35.71%) (p < 0.001). One (7.14%) case of progression to furcate cord insertion due to haematoma at the root of the umbilical cord ended with an emergency caesarean section. In terms of perinatal complications, marginal cord insertion that progressed to furcate cord insertion had higher incidences of SGA infants, abnormal placental morphology, retention of the placenta, and cord-related adverse pregnancy outcomes than not progressed to furcate cord insertion (p < 0.05).
Marginal cord insertion in the first trimester has the potential to progress to furcate cord insertion. We suggest that ultrasound-diagnosed marginal cord insertion in the first trimester should be watched carefully in the second trimester, which is clinically useful to accurately determine the category of cord insertion and to improve the rate of prenatal diagnosis of furcate cord insertion.
评估妊娠早期边缘脐带插入与妊娠后期分叉脐带插入之间的潜在联系。
这是一项对 3178 例单胎妊娠的脐带插入部位筛查数据进行的前瞻性研究。脐带插入部位分两阶段检查。第一阶段是在妊娠 10-13 周时筛查脐带插入部位,目的是确定脐带插入类别。第二阶段在妊娠 22-28 周进行,以随访脐带插入部位与胎盘之间的关系,并确定脐带插入类别的任何变化。通过识别脐带主干在到达胎盘之前是否分离或分支来诊断或排除分叉脐带插入。评估影响分叉脐带插入进展和围产期并发症的因素。
14 例(0.44%)进展为分叉脐带插入,所有病例在妊娠早期超声检查均显示边缘脐带插入(p<0.001)。在没有进展为分叉脐带插入的 3050 例(96.40%)中,与早期妊娠相比,脐带插入类别无变化。114 例(3.60%)脐带插入类别变化与分叉脐带插入不一致。共有 14 例进展为分叉脐带插入,所有病例脐带插入部位均紧密相邻,其中 11 例(78.57%)为低插入部位(p<0.001)。关于分娩方式的选择,行选择性剖宫产术 8 例(57.14%)。自然阴道分娩率为 5/14(35.71%)(p<0.001)。1 例(7.14%)因脐带根部血肿进展为分叉脐带插入,行急症剖宫产术。在围产期并发症方面,进展为分叉脐带插入的边缘脐带插入胎儿生长受限、胎盘形态异常、胎盘滞留和脐带相关不良妊娠结局的发生率高于未进展为分叉脐带插入者(p<0.05)。
妊娠早期边缘脐带插入有进展为分叉脐带插入的可能。我们建议,在妊娠中期应仔细观察妊娠早期超声诊断的边缘脐带插入,这对于准确确定脐带插入类别和提高分叉脐带插入的产前诊断率具有临床意义。