Department of Endocrinology and Nutrition, Hospital del Mar, Passeig Marítim, 25-29, Barcelona, 08003, Spain.
Department of Medicine, Universitat Pompeu Fabra, Plaça de la Mercè, 10-12, Barcelona, 08002, Spain.
Cardiovasc Diabetol. 2024 Jun 15;23(1):205. doi: 10.1186/s12933-024-02296-x.
There has been a substantial increase in the use of laparoscopic sleeve gastrectomy (SG) to treat morbid obesity despite observational evidence demonstrating the superiority of Roux-en-Y gastric bypass (RYGB) for reducing low-density lipoprotein (LDL) cholesterol. The main aim was to ascertain whether high LDL cholesterol levels should be considered when selecting the most appropriate surgical procedure for each patient (RYGB or SG).
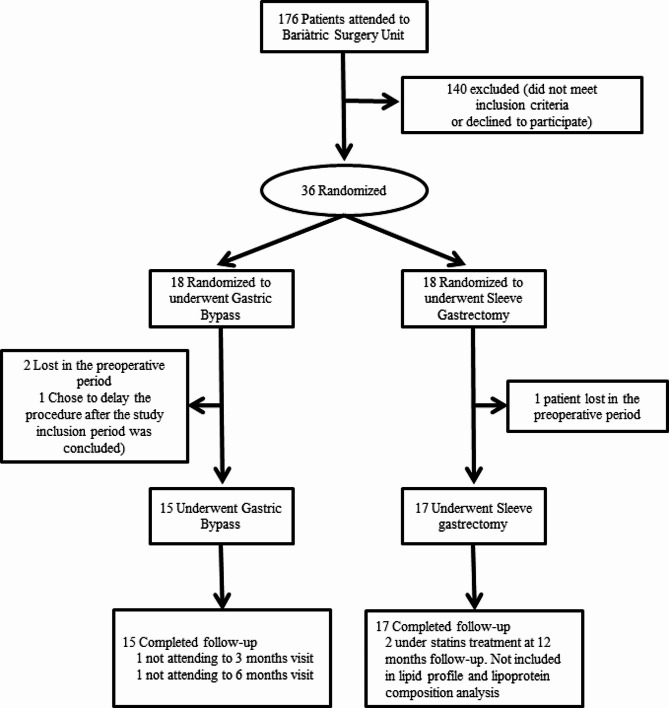
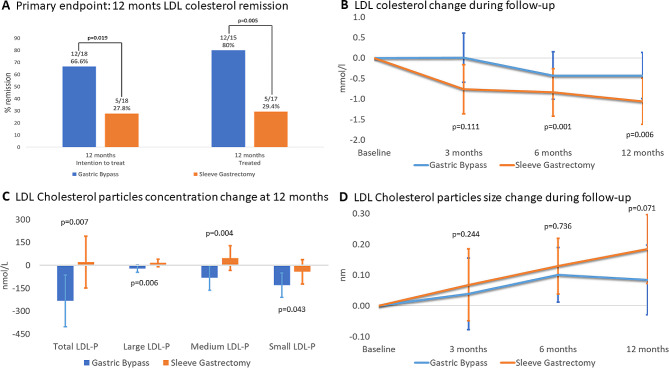
In this single-center, randomized clinical trial using intention-to-treat analysis, 38 patients with severe obesity and elevated levels of LDL cholesterol were randomly assigned to undergo RYGB or SG. The primary outcome was LDL cholesterol remission at 12 months, defined as LDL cholesterol < 3.36 nmol/l without lipid-lowering medications. Secondary outcomes included changes in weight, other comorbidities, qualitative lipoprotein traits, cholesterol esters, glycoproteins, cholesterol absorption and synthesis metabolites and complications.
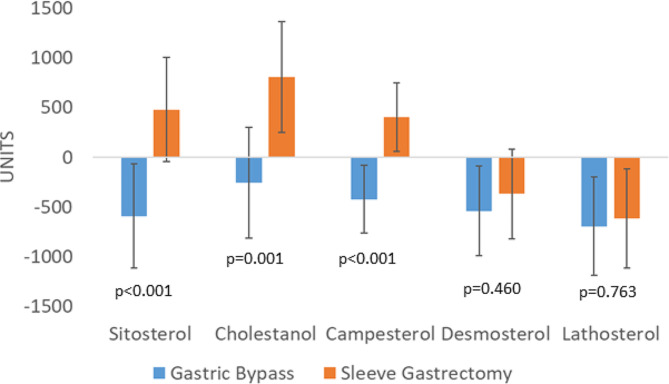
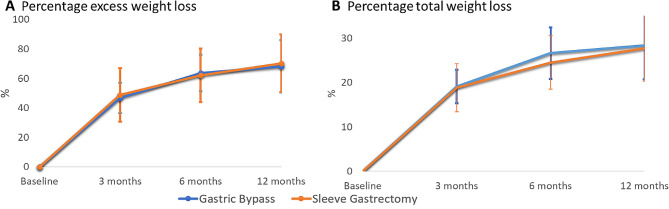
Intention-to-treat analysis revealed that LDL cholesterol remission occurred in 66.6% of RYGB patients compared to 27.8% of SG patients (p = 0.019). Among patients completing follow-up, RYGB demonstrated superior remission (80.0% vs. 29.4%, p = 0.005). Exclusive benefits of RYGB included a reduction in large, medium, and small LDL particles. Cholesterol absorption markers showed differential behavior after both techniques: campesterol (Δ -15.2 µg/mg, 95% CI -30.2 to -0.1) decreased after RYGB, and sitosterol (Δ 21.1 µg/mg, 95% CI 0.9 to 41.2), cholestanol (Δ 30.6 µg/mg, 95% CI 14.8 to 57.9) and campesterol (Δ 18.4 µg/mg, 95% CI 4.4 to 32.3) increased after SG. No differences in weight loss, cholesterol esters, glycoproteins, cholesterol synthesis metabolites or postoperative complications were observed between techniques.
In conclusion, RYGB is superior to SG in terms of short-term of high LDL cholesterol remission. Furthermore, RYGB also led to a greater improvement in lipoprotein parameters that confer an atherogenic profile. Therefore, the presence of elevated levels of LDL cholesterol should be considered when determining the optimal bariatric surgery procedure for each patient.
Clinicaltrials.gov number, NCT03975478).
尽管观察性证据表明 Roux-en-Y 胃旁路术(RYGB)在降低低密度脂蛋白(LDL)胆固醇方面更具优势,但腹腔镜袖状胃切除术(SG)治疗病态肥胖的应用仍显著增加。主要目的是确定在为每位患者选择最合适的手术程序(RYGB 或 SG)时,是否应考虑高 LDL 胆固醇水平。
在这项采用意向治疗分析的单中心随机临床试验中,38 名患有严重肥胖症和 LDL 胆固醇升高的患者被随机分配接受 RYGB 或 SG。主要结局是 12 个月时 LDL 胆固醇缓解,定义为 LDL 胆固醇<3.36 nmol/l 且无需降脂药物治疗。次要结局包括体重变化、其他合并症、定性脂蛋白特征、胆固醇酯、糖蛋白、胆固醇吸收和合成代谢物以及并发症。
意向治疗分析显示,RYGB 患者中 LDL 胆固醇缓解率为 66.6%,而 SG 患者为 27.8%(p=0.019)。在完成随访的患者中,RYGB 显示出更好的缓解(80.0% vs. 29.4%,p=0.005)。RYGB 的独特益处包括大、中、小 LDL 颗粒的减少。胆固醇吸收标志物在两种技术后表现出不同的行为:RYGB 后胆固醇甾醇(Δ-15.2μg/mg,95%CI-30.2 至-0.1)减少,而谷甾醇(Δ21.1μg/mg,95%CI0.9 至 41.2)、菜油甾醇(Δ30.6μg/mg,95%CI14.8 至 57.9)和胆固醇甾醇(Δ18.4μg/mg,95%CI4.4 至 32.3)增加。两种技术之间在体重减轻、胆固醇酯、糖蛋白、胆固醇合成代谢物或术后并发症方面没有差异。
总之,RYGB 在短期内对高 LDL 胆固醇缓解方面优于 SG。此外,RYGB 还导致脂蛋白参数的更大改善,从而产生致动脉粥样硬化的特征。因此,在确定每位患者最佳减重手术程序时,应考虑 LDL 胆固醇水平升高的情况。
Clinicaltrials.gov 编号,NCT03975478)。