Ambrogi Marcello Carlo, Aprile Vittorio, Sanna Stefano, Forti Parri Sergio Nicola, Rizzardi Giovanna, Fanucchi Olivia, Valentini Leonardo, Italiani Alberto, Morganti Riccardo, Cartia Carlotta Francesca, Hughes James M, Lucchi Marco, Droghetti Andrea
Department for Surgical, Medical, Molecular Pathology and Critical Care, University of Pisa, 56124 Pisa, Italy.
Division of Thoracic Surgery, University Hospital of Pisa, 56124 Pisa, Italy.
J Clin Med. 2024 May 25;13(11):3106. doi: 10.3390/jcm13113106.
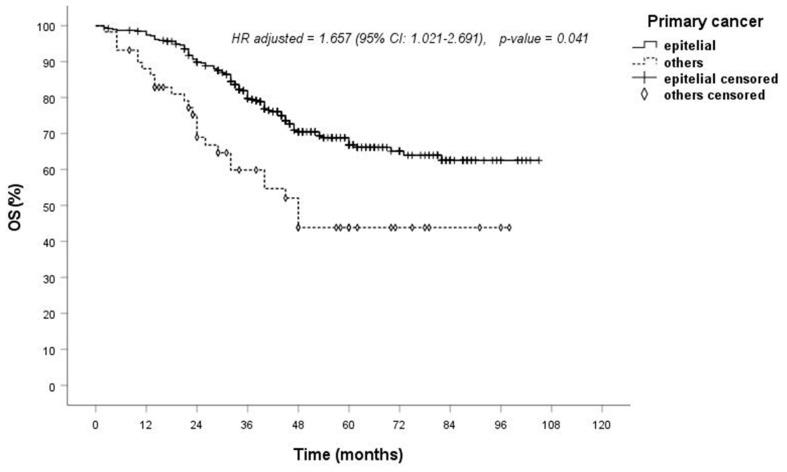
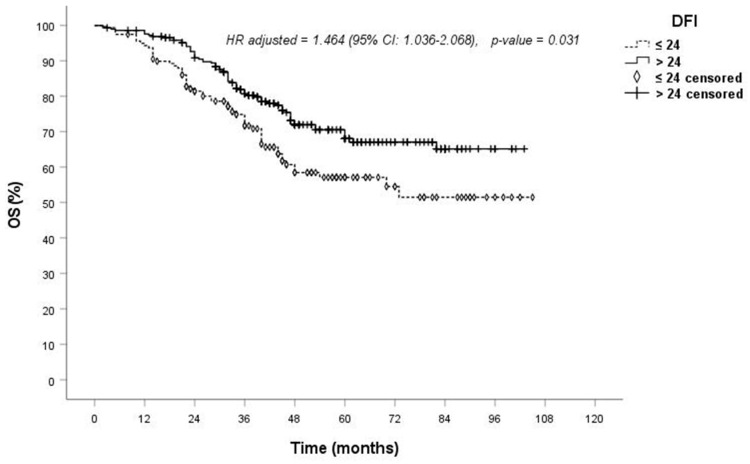
: The surgical resection of pulmonary metastases is considered a therapeutic option in selected cases. In light of this, we present the results from a national multicenter prospective registry of lung metastasectomy. : This retrospective analysis involves data collected prospectively and consecutively in a national multicentric Italian database, including patients who underwent lung metastasectomy. The primary endpoints were the analysis of morbidity and overall survival (OS), with secondary endpoints focusing on the analysis of potential risk factors affecting both morbidity and OS. : A total 470 lung procedures were performed (4 pneumonectomies, 46 lobectomies/bilobectomies, 13 segmentectomies and 407 wedge resections) on 461 patients (258 men and 203 women, mean age of 63.1 years). The majority of patients had metastases from colorectal cancer (45.8%). In most cases (63.6%), patients had only one lung metastasis. A minimally invasive approach was chosen in 143 cases (30.4%). The mean operative time was 118 min, with no reported deaths. Morbidity most frequently consisted of prolonged air leaking and bleeding, but no re-intervention was required. Statistical analysis revealed that morbidity was significantly affected by operative time and pulmonary comorbidities, while OS was significantly affected by disease-free interval (DFI) > 24 months ( = 0.005), epithelial histology ( = 0.001) and colorectal histology ( = 0.004) during univariate analysis. No significant correlation was found between OS and age, gender, surgical approach, surgical extent, surgical device, the number of resected metastases, lesion diameter, the site of lesions and nodal involvement. Multivariate analysis of OS confirmed that only epithelial histology and DFI were risk-factors, with -values of 0.041 and 0.031, respectively. : Lung metastasectomy appears to be a safe procedure, with acceptable morbidity, even with a minimally invasive approach. However, it remains a local treatment of a systemic disease. Therefore, careful attention should be paid to selecting patients who could truly benefit from surgical intervention.
在特定病例中,肺转移瘤的手术切除被视为一种治疗选择。鉴于此,我们展示了一项全国多中心肺转移瘤切除术前瞻性登记研究的结果。
这项回顾性分析涉及在意大利全国多中心数据库中前瞻性且连续收集的数据,包括接受肺转移瘤切除术的患者。主要终点是分析发病率和总生存期(OS),次要终点集中于分析影响发病率和OS的潜在风险因素。
共对461例患者(258例男性和203例女性,平均年龄63.1岁)进行了470例肺部手术(4例全肺切除术、46例肺叶切除术/双肺叶切除术、13例肺段切除术和407例楔形切除术)。大多数患者的转移瘤来自结直肠癌(45.8%)。在大多数病例(63.6%)中,患者仅有一个肺转移瘤。143例(30.4%)采用了微创方法。平均手术时间为118分钟,无死亡报告。发病率最常见的是持续漏气和出血,但无需再次干预。统计分析显示,发病率受手术时间和肺部合并症的显著影响,而在单因素分析中,OS受无病间期(DFI)>24个月(P = 0.005)、上皮组织学(P = 0.001)和结直肠组织学(P = 0.004)的显著影响。未发现OS与年龄、性别、手术方式、手术范围、手术器械、切除转移瘤的数量、病变直径、病变部位和淋巴结受累之间存在显著相关性。OS的多因素分析证实,只有上皮组织学和DFI是危险因素,P值分别为0.041和0.031。
肺转移瘤切除术似乎是一种安全的手术,发病率可接受,即使采用微创方法。然而,它仍然是对全身性疾病的局部治疗。因此,应谨慎选择真正能从手术干预中获益的患者。