Poonsombudlert Kittika, Mott Sarah, Miller Benda, Yodsuwan Ratdanai, Shaikh Hira, Strouse Christopher, Lochner Jonathan, Farooq Umar, Magalhaes-Silverman Margarida
Holden Comprehensive Cancer at the University of Iowa Hospitals and Clinics Iowa City Iowa USA.
EJHaem. 2024 Apr 28;5(3):578-583. doi: 10.1002/jha2.909. eCollection 2024 Jun.
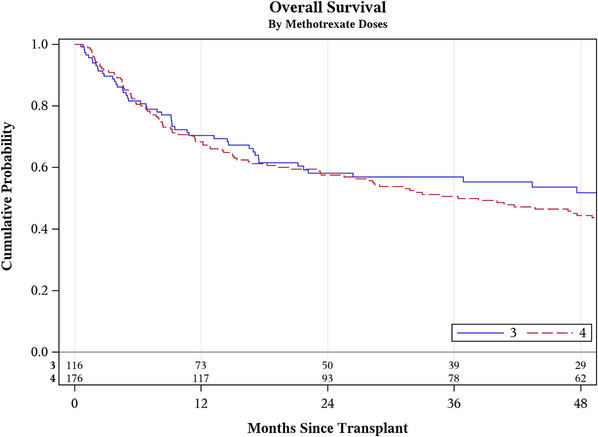
Methotrexate (MTX) doses on days +1, +3, +6, and +11 after match unrelated donor allogeneic stem cell transplant (MUD HSCT) is a common graft-versus-host disease (GVHD) prophylaxis regimen. However, the overlapping toxicity of MTX with conditioning chemotherapy sometimes warrants the omission of the fourth dose of MTX. Prior single-institution studies showed conflicting results comparing the outcomes of patients who received three versus four doses of MTX, but to our knowledge, the effect of concomitant antithymocyte globulin (ATG) has not been reported. Charts of patients who underwent MUD HSCT between 2009 and 2023 were reviewed. Patients received rabbit ATG (Thymoglobulin), given at 0.5 mg/kg on day -3, 2 mg/kg on day -2, and 2.5 mg/kg on day -1. MTX is given at 15 mg/m on day +1 and 10 mg/m on days +3, +6, and +11. Severe mucositis was the most common indication for day +11 MTX omission (82%). We identified 292 patients (116 in 3 dose cohort and 176 in 4 dose cohort). Median follow-up was 23 months (range 1-151). Patients in the 4 doses cohort were more frequently male (68% vs. 50%, < 0.01), received a reduced intensity conditioning regimen (38.0% vs. 22%, < 0.01), were older (median 58 vs. 54 years, = 0.02), and received a transplant in the earlier era (median HSCT year 2014 vs. 2018, < 0.01). A statistically significant difference was not evidenced between the cohorts for the following outcomes: acute GVHD (aGVHD) (HR 1.1, 95% CI 0.9-1.5), chronic GVHD (cGVHD) (HR 1.3, 95% CI 0.8-1.6), relapse-free survival (RFS) (HR 1.0, 95% CI 0.6-1.5), non-relapse mortality (NRM) (HR 1.4, 95% CI 0.9-2.2), and overall survival (OS) (HR 1.2, 95% CI 0.9-1.7). Both cohorts had similar median time to neutrophil engraftment at 14 days. When ATG is incorporated, omission of day +11 MTX does not significantly impact the rate of engraftment or cumulative incidence of aGVHD, cGVHD, RFS, NRM, and OS.
在非血缘供者异基因造血干细胞移植(MUD HSCT)后第1、3、6和11天使用甲氨蝶呤(MTX)是一种常见的移植物抗宿主病(GVHD)预防方案。然而,MTX与预处理化疗的重叠毒性有时需要省略MTX的第四剂。先前的单中心研究在比较接受三剂与四剂MTX的患者结局时结果相互矛盾,但据我们所知,尚未报道同时使用抗胸腺细胞球蛋白(ATG)的效果。回顾了2009年至2023年间接受MUD HSCT的患者病历。患者接受兔ATG(即复宁),在第-3天给予0.5mg/kg,第-2天给予2mg/kg,第-1天给予2.5mg/kg。MTX在第+1天给予15mg/m²,在第+3、+6和11天给予10mg/m²。严重黏膜炎是第11天省略MTX最常见的原因(82%)。我们确定了292例患者(三剂组116例,四剂组176例)。中位随访时间为23个月(范围1 - 151个月)。四剂组患者男性比例更高(68%对50%,P<0.01),接受减低强度预处理方案的比例更高(38.0%对22%,P<0.01),年龄更大(中位年龄58岁对54岁,P = 0.02),且在更早的时期接受移植(HSCT中位年份2014年对2018年,P<0.01)。在以下结局方面,两组之间未发现统计学显著差异:急性移植物抗宿主病(aGVHD)(风险比1.1,95%置信区间0.9 - 1.5)、慢性移植物抗宿主病(cGVHD)(风险比1.3,95%置信区间0.8 - 1.6)、无复发生存期(RFS)(风险比1.0,95%置信区间0.6 - 1.5)、非复发死亡率(NRM)(风险比1.4,95%置信区间0.9 - 2.2)和总生存期(OS)(风险比1.2,95%置信区间0.9 - 1.7)。两组中性粒细胞植入的中位时间均为14天。当加入ATG时,省略第11天的MTX不会显著影响植入率或aGVHD、cGVHD、RFS、NRM和OS的累积发生率。