Groothof Dion, Shehab Naser B N, Erler Nicole S, Post Adrian, Kremer Daan, Polinder-Bos Harmke A, Gansevoort Ron T, Groen Henk, Pol Robert A, Gans Reinold O B, Bakker Stephan J L
Department of Internal Medicine, Division of Nephrology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands.
Department of Biostatistics, Erasmus Medical Center, Erasmus University Rotterdam, Rotterdam, the Netherlands.
J Cachexia Sarcopenia Muscle. 2024 Aug;15(4):1528-1538. doi: 10.1002/jcsm.13511. Epub 2024 Jun 19.
Serum creatinine is used as initial test to derive eGFR and confirmatory testing with serum cystatin C is recommended when creatinine-based eGFR is considered less accurate due to deviant muscle mass. Low muscle mass is associated with increased risk of premature mortality. However, the associations of serum creatinine and cystatin C with muscle mass and mortality remain unclear and require further investigation to better inform clinical decision-making.
We included 8437 community-dwelling adults enrolled in the Dutch PREVEND study and 5033 in the US NHANES replication cohort. Associations of serum creatinine and/or cystatin C with muscle mass surrogates and mortality were quantified with linear and Cox proportional hazards regression, respectively. Missing observations in covariates were multiply imputed using Substantive Model Compatible Fully Conditional Specification.
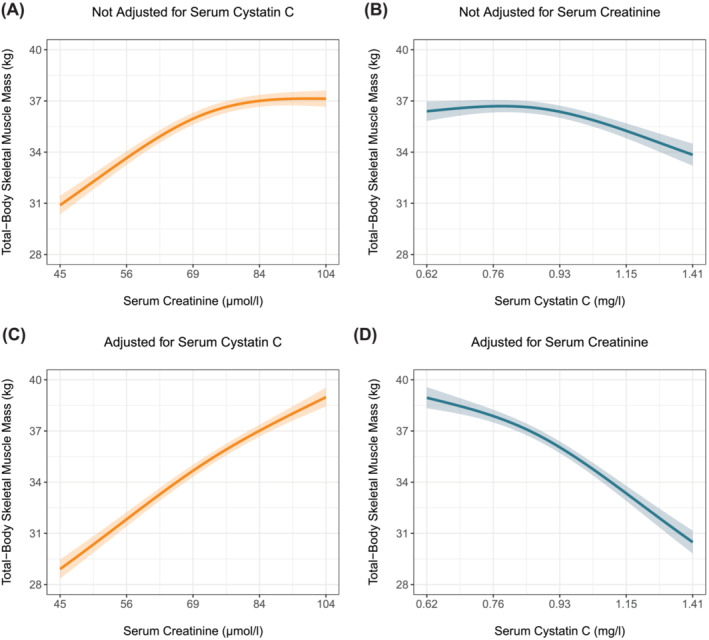
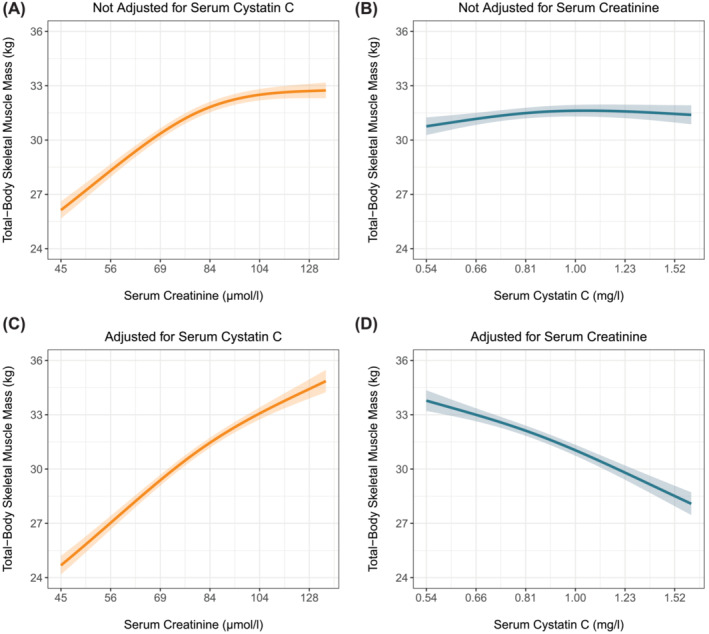
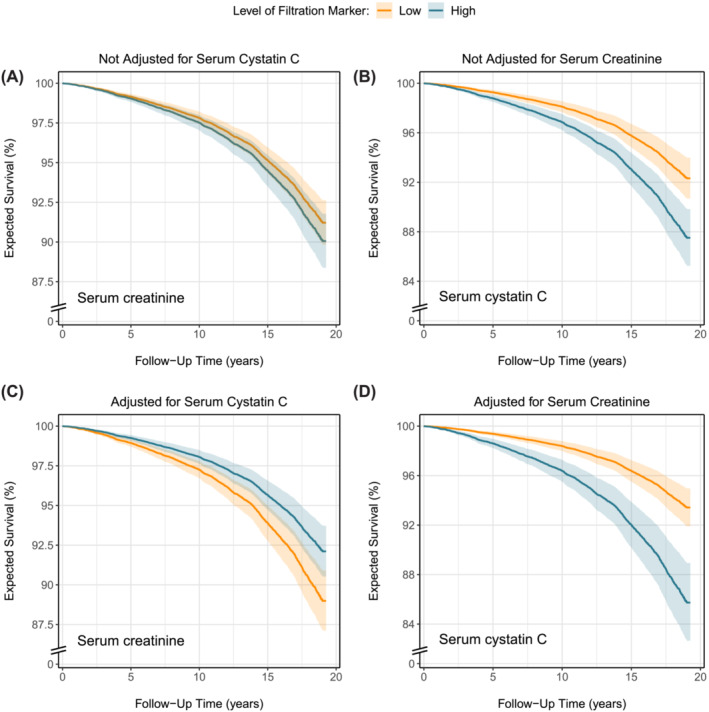
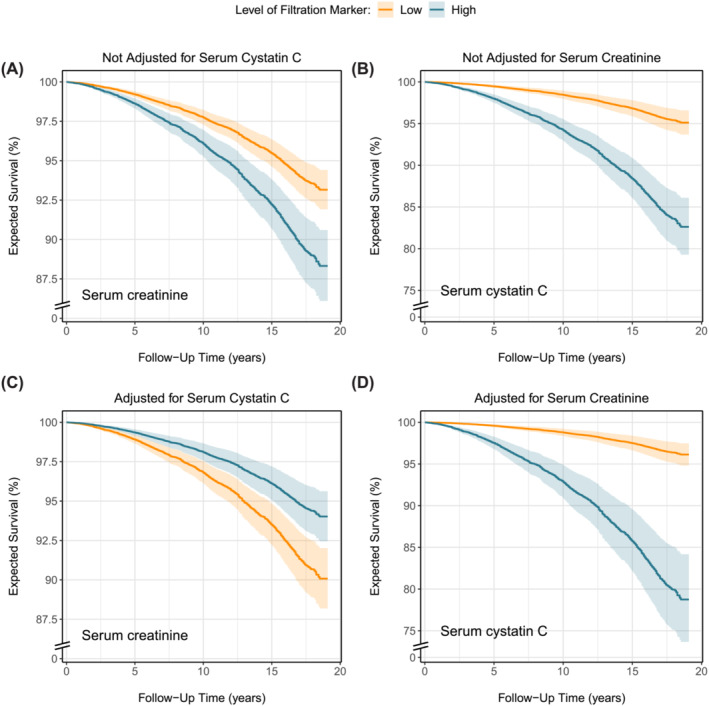
Mean (SD) age of PREVEND and NHANES participants (50% and 48% male) were 49.8 (12.6) and 48.7 (18.7) years, respectively. Median (Q1-Q3) serum creatinine and cystatin C were 71 (61-80) and 80 (62-88) μmol/L and 0.87 (0.78-0.98) and 0.91 (0.80-1.10) mg/L, respectively. Higher serum creatinine was associated with greater muscle mass, while serum cystatin C was not associated with muscle mass. Adjusting both markers for each other strengthened the positive relationship between serum creatinine and muscle mass and revealed an inverse association between serum cystatin C and muscle mass. In the PREVEND cohort, 1636 (19%) deaths were registered over a median follow-up of 12.9 (5.8-16.3) years with a 10-year mortality rate (95% CI) of 7.6% (7.1-8.2%). In the NHANES, 1273 (25%) deaths were registered over a median follow-up of 17.9 (17.3-18.5) years with a 10-year mortality rate of 13.8% (12.8-14.7%). Both markers were associated with increased mortality. Notably, when adjusted for each other, higher serum creatinine was associated with decreased mortality, while the association between serum cystatin C and increased mortality strengthened. The shapes of the associations in the PREVEND study and NHANES were almost identical.
The strong association between serum creatinine and muscle mass challenges its reliability as GFR marker, necessitating a more cautious approach in its clinical use. The minimal association between serum cystatin C and muscle mass supports its increased use as a more reliable alternative in routine clinical practice.
血清肌酐用作估算肾小球滤过率(eGFR)的初始检测指标,当基于肌酐的eGFR因肌肉量异常而被认为准确性较差时,建议用血清胱抑素C进行验证性检测。低肌肉量与过早死亡风险增加相关。然而,血清肌酐和胱抑素C与肌肉量及死亡率之间的关联仍不明确,需要进一步研究以更好地为临床决策提供依据。
我们纳入了荷兰预防和延缓肾病发展(PREVEND)研究中的8437名社区居住成年人以及美国国家健康与营养检查调查(NHANES)重复队列中的5033名成年人。分别用线性回归和Cox比例风险回归对血清肌酐和/或胱抑素C与肌肉量替代指标及死亡率之间的关联进行量化。协变量中的缺失观测值使用实质模型兼容完全条件设定进行多重填补。
PREVEND和NHANES参与者的平均(标准差)年龄(男性分别占50%和48%)分别为49.8(12.6)岁和48.7(18.7)岁。血清肌酐和胱抑素C的中位数(四分位间距)分别为71(61 - 80)μmol/L和80(62 - 88)μmol/L,以及0.87(0.78 - 0.98)mg/L和0.91(0.80 - 1.10)mg/L。较高的血清肌酐与更大的肌肉量相关,而血清胱抑素C与肌肉量无关。相互调整这两个指标后,血清肌酐与肌肉量之间的正相关关系增强,且显示血清胱抑素C与肌肉量呈负相关。在PREVEND队列中,在中位随访12.9(5.8 - 16.3)年期间记录了1636例(19%)死亡,10年死亡率(95%置信区间)为7.6%(7.1 - 8.2%)。在NHANES中,在中位随访17.9(17.3 - 18.5)年期间记录了1273例(25%)死亡,10年死亡率为13.8%(12.8 - 14.7%)。这两个指标均与死亡率增加相关。值得注意的是,相互调整后,较高的血清肌酐与死亡率降低相关,而血清胱抑素C与死亡率增加之间的关联增强。PREVEND研究和NHANES中关联的形状几乎相同。
血清肌酐与肌肉量之间的强关联对其作为肾小球滤过率标志物的可靠性提出了挑战,在临床应用中需要采取更谨慎的方法。血清胱抑素C与肌肉量之间的关联极小,支持其在常规临床实践中作为更可靠的替代指标增加使用。