Prytula Agnieszka, Shroff Rukshana, van Gremberghe Ineke, Krupka Kai, Bacchetta Justine, Benetti Elisa, Grenda Ryszard, Guzzo Isabella, Kanzelmeyer Nele, Büyükkaragöz Bahar, Kranz Birgitta, Nalçacıoğlu Hülya, Oh Jun, Pape Lars, Shenoy Mohan, Sellier-Leclerc Anne-Laure, Tönshoff Burkhard
Department of Pediatric Nephrology and Rheumatology, Ghent University Hospital, Belgium.
Renal Unit, UCL Great Ormond Street Hospital, London, UK.
Kidney Int Rep. 2024 Apr 8;9(6):1684-1693. doi: 10.1016/j.ekir.2024.04.007. eCollection 2024 Jun.
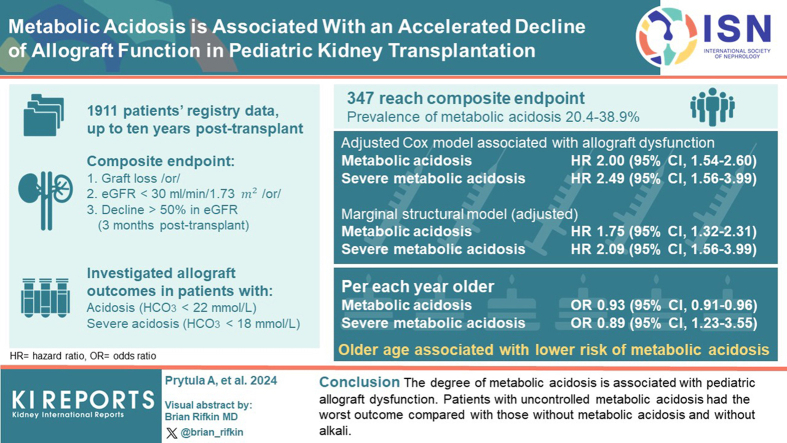
We investigated the relationship between metabolic acidosis over time and allograft outcome in pediatric kidney transplantation (KTx).
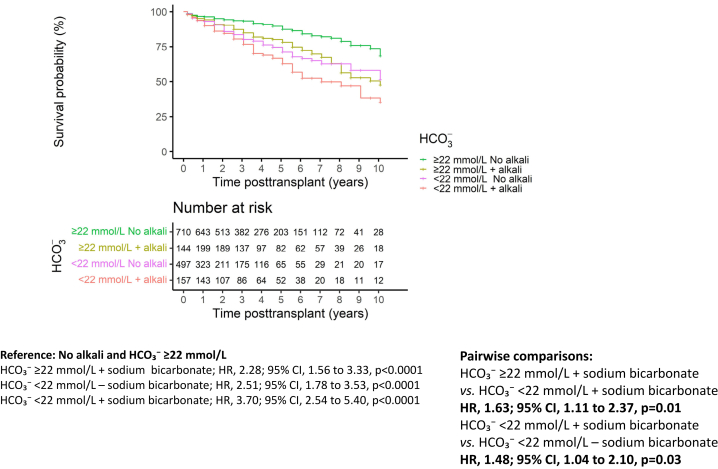
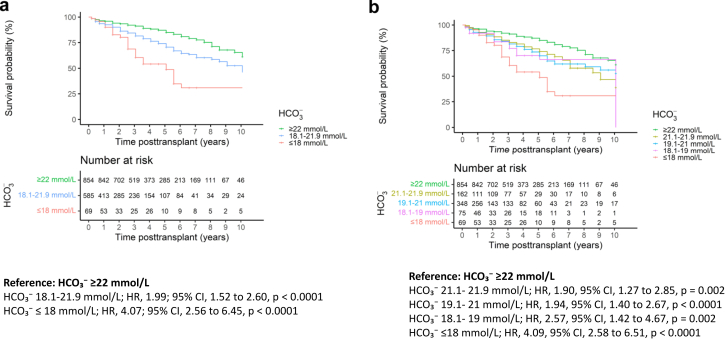
This registry study collected data up to 10 years posttransplant. Survival analysis for a composite end point of graft loss or estimated glomerular filtration rate (eGFR) ≤ 30 ml/min per 1.73 m or ≥50% decline from eGFR at month 3 posttransplant was performed. The association of serum bicarbonate concentration (HCO ) < 22 mmol/l (metabolic acidosis) and HCO < 18 mmol/l (severe metabolic acidosis) with allograft outcome was investigated using stratified Cox models and marginal structural models. Secondary analyses included the identification of risk factors for metabolic acidosis and the relationship between alkali supplementation and allograft outcome.
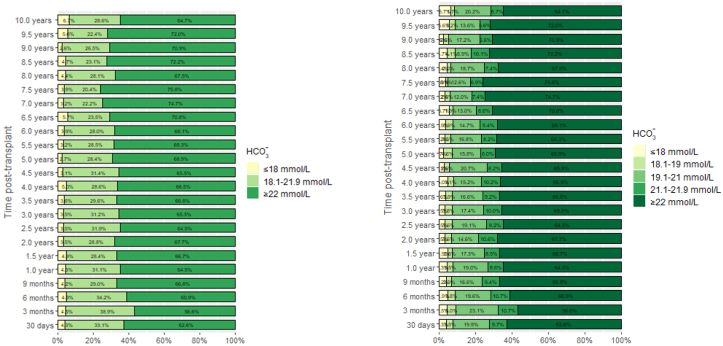
We report on 1911 patients, of whom 347 reached the composite end point. The prevalence of metabolic acidosis over time ranged from 20.4% to 38.9%. In the adjusted Cox models, metabolic acidosis (hazard ratio [HR], 2.00; 95% confidence interval [CI], 1.54-2.60) and severe metabolic acidosis (HR, 2.49; 95% CI, 1.56-3.99) were associated with allograft dysfunction. Marginal structural models showed similar results (HR, 1.75; 95% CI, 1.32-2.31 and HR, 2.09; 95% CI, 1.23-3.55, respectively). Older age was associated with a lower risk of metabolic acidosis (odds ratio [OR] 0.93/yr older; 95% CI, 0.91-0.96) and severe metabolic acidosis (OR, 0.89; 95% CI, 0.84-0.95). Patients with uncontrolled metabolic acidosis had the worst outcome compared to those without metabolic acidosis and without alkali (HR, 3.70; 95% CI, 2.54-5.40).
The degree of metabolic acidosis is associated with allograft dysfunction.
我们研究了小儿肾移植(KTx)中代谢性酸中毒随时间的变化与同种异体移植结局之间的关系。
这项登记研究收集了移植后长达10年的数据。对移植失败或估计肾小球滤过率(eGFR)≤30 ml/(min·1.73 m²)或较移植后3个月时的eGFR下降≥50%这一复合终点进行生存分析。使用分层Cox模型和边际结构模型研究血清碳酸氢盐浓度(HCO₃⁻)<22 mmol/L(代谢性酸中毒)和HCO₃⁻<18 mmol/L(严重代谢性酸中毒)与同种异体移植结局的关联。二级分析包括确定代谢性酸中毒的危险因素以及碱补充与同种异体移植结局之间的关系。
我们报告了1911例患者,其中347例达到复合终点。代谢性酸中毒随时间的发生率在20.4%至38.9%之间。在调整后的Cox模型中,代谢性酸中毒(风险比[HR],2.00;95%置信区间[CI],1.54 - 2.60)和严重代谢性酸中毒(HR,2.49;95% CI,1.56 - 3.99)与同种异体移植功能障碍相关。边际结构模型显示了相似的结果(HR分别为1.75;95% CI,1.32 - 2.31和HR,2.09;95% CI,1.23 - 3.55)。年龄较大与代谢性酸中毒(优势比[OR] 每大1岁为0.93;95% CI,0.91 - 0.96)和严重代谢性酸中毒(OR,0.89;95% CI,0.84 - 0.95)的风险较低相关。与没有代谢性酸中毒且未补充碱的患者相比,代谢性酸中毒未得到控制的患者结局最差(HR,3.70;95% CI,2.54 - 5.40)。
代谢性酸中毒的程度与同种异体移植功能障碍相关。