Department of Internal Medicine, Institute of Kidney Disease Research, Yonsei University College of Medicine, Seoul, Republic of Korea.
Department of Internal Medicine, International Saint Mary's Hospital, Catholic Kwandong University, Incheon, Republic of Korea.
Sci Rep. 2024 Jun 21;14(1):14284. doi: 10.1038/s41598-024-64224-z.
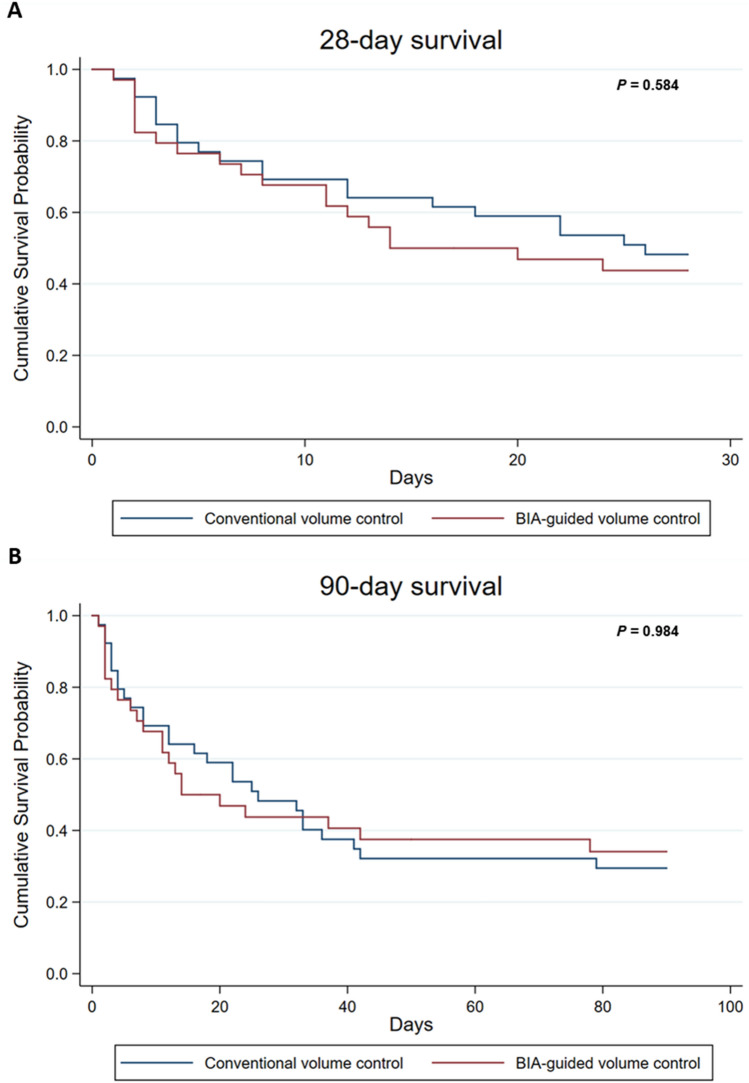
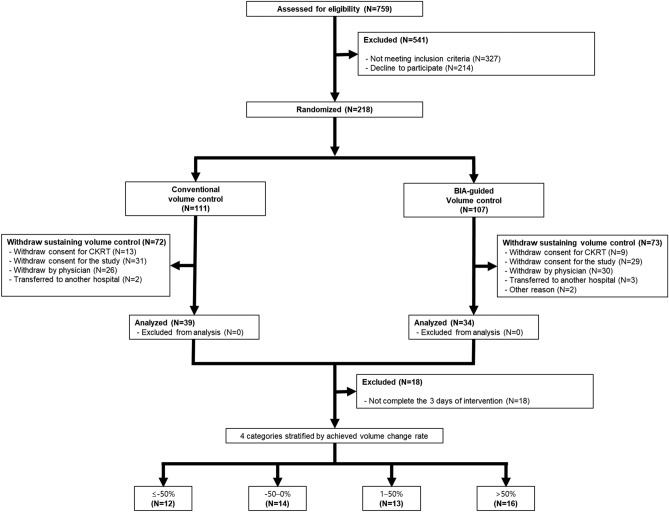
Optimal strategy for volume control and the clinical implication of achieved volume control are unknown in patients with sepsis-associated acute kidney injury (AKI) receiving continuous renal replacement therapy (CRRT). This randomized controlled trial aimed to compare the survival according to conventional or bioelectrical impedance analysis (BIA)-guided volume control strategy in patients with sepsis-associated AKI receiving CRRT. We also compared patient survival according to achieved volume accumulation rate ([cumulative fluid balance during 3 days × 100]/fluid overload measured by BIA at enrollment) as a post-hoc analysis. We randomly assigned patients to conventional volume control strategy (n = 39) or to BIA-guided volume control strategy (n = 34). There were no differences in 28-day mortality (HR, 1.19; 95% CI, 0.63-2.23) or 90-day mortality (HR, 0.99; 95% CI 0.57-1.75) between conventional and BIA-guided volume control group. In the secondary analysis, achieved volume accumulation rate was significantly associated with patient survival. Compared with the achieved volume accumulation rate of ≤ - 50%, the HRs (95% CIs) for the risk of 90-day mortality were 1.21 (0.29-5.01), 0.55 (0.12-2.48), and 7.18 (1.58-32.51) in that of - 50-0%, 1-50%, and > 50%, respectively. Hence, BIA-guided volume control in patients with sepsis-associated AKI receiving CRRT did not improve patient outcomes. In the secondary analysis, achieved volume accumulation rate was associated with patient survival.
在接受连续性肾脏替代治疗(CRRT)的脓毒症相关急性肾损伤(AKI)患者中,容量控制的最佳策略以及实现的容量控制的临床意义尚不清楚。本随机对照试验旨在比较接受 CRRT 的脓毒症相关 AKI 患者中,常规或生物电阻抗分析(BIA)指导的容量控制策略的生存情况。我们还根据达到的容量累积率([第 3 天的累积液体平衡量×100]/在入组时 BIA 测量的液体超负荷)进行了事后分析,比较了患者的生存情况。我们将患者随机分配到常规容量控制策略组(n=39)或 BIA 指导的容量控制策略组(n=34)。两组的 28 天死亡率(HR,1.19;95%CI,0.63-2.23)或 90 天死亡率(HR,0.99;95%CI,0.57-1.75)均无差异。在次要分析中,达到的容量累积率与患者的生存显著相关。与达到的容量累积率≤-50%相比,达到的容量累积率为-50-0%、1-50%和>50%时,90 天死亡率的 HR(95%CI)分别为 1.21(0.29-5.01)、0.55(0.12-2.48)和 7.18(1.58-32.51)。因此,在接受 CRRT 的脓毒症相关 AKI 患者中,BIA 指导的容量控制并不能改善患者的结局。在次要分析中,达到的容量累积率与患者的生存相关。