Department of Pediatric Oncology, Erasmus MC-Sophia Children's Hospital Rotterdam, Wytemaweg 80, 3015 CN, Rotterdam, The Netherlands.
Princess Máxima Center for Pediatric Oncology, Utrecht, The Netherlands.
Clin Pharmacokinet. 2024 Jul;63(7):981-997. doi: 10.1007/s40262-024-01386-z. Epub 2024 Jun 22.
Inotuzumab ozogamicin is an antibody-drug conjugate approved for treating relapsed/refractory B-cell precursor acute lymphoblastic leukemia (BCP-ALL) in adults. Pediatric pharmacokinetic data of inotuzumab ozogamicin are lacking. This study is the first to examine the population pharmacokinetics of inotuzumab ozogamicin in pediatric patients with relapsed/refractory BCP-ALL.
From 531 adult patients with B-cell non-Hodgkin's lymphoma, 234 adult patients with BCP-ALL, and 53 pediatric patients with BCP-ALL, 8924 inotuzumab ozogamicin serum concentrations were analyzed using non-linear mixed-effects modeling. A published adult inotuzumab ozogamicin population-pharmacokinetic model, a two-compartment model with linear and time-dependent clearance, was adapted to describe the pediatric data.
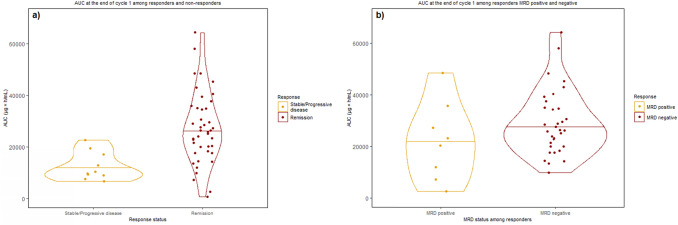
Modifications in this analysis, compared to the published adult model, included: (i) re-estimating pharmacokinetic parameters and covariate effects; (ii) modifying covariate representation; and (iii) introducing relevant pediatric covariate effects (age on the decay coefficient of time-dependent clearance and ALL effect (disease type and/or different bioanalytical analysis methods) on initial values of time-dependent clearance). For patients with relapsed/refractory BCP-ALL, increasing age was associated with a decreasing decay coefficient of time-dependent clearance, reflecting that the target-mediated drug clearance declines more rapidly in children. In pediatric BCP-ALL, the median [interquartile range] cumulative area under the concentration-time curve was significantly higher among responders (n = 42) versus non-responders (n = 10) at the end of the first cycle (26.1 [18.9-35.0] vs 10.1 [9.19-16.1], × 10 ng*h/mL, p < 0.001). From simulations performed at the recommended pediatric phase II dose, inotuzumab ozogamicin exposure reached a similar level as observed in responding pediatric trial participants.
The pharmacokinetic profile of inotuzumab ozogamicin in pediatric patients with relapsed/refractory BCP-ALL was well described in this study. No dose adjustment is required clinically for pediatric patients with BCP-ALL based on the simulated inotuzumab ozogamicin exposure at the recommended pediatric phase II dose, promising efficacy and acceptable tolerability.
依妥珠单抗奥佐米星是一种抗体-药物偶联物,已被批准用于治疗成人复发/难治性 B 细胞前体急性淋巴细胞白血病(BCP-ALL)。儿科患者的依妥珠单抗奥佐米星药代动力学数据尚缺乏。本研究首次对复发/难治性 BCP-ALL 儿科患者的依妥珠单抗奥佐米星群体药代动力学进行了研究。
从 531 例 B 细胞非霍奇金淋巴瘤成人患者、234 例 BCP-ALL 成人患者和 53 例 BCP-ALL 儿科患者中,共分析了 8924 例依妥珠单抗奥佐米星血清浓度,采用非线性混合效应模型进行分析。采用已发表的成人依妥珠单抗奥佐米星群体药代动力学模型,即一个具有线性和时间依赖性清除的两室模型,对儿科数据进行描述。
与已发表的成人模型相比,本分析的修改包括:(i)重新估计药代动力学参数和协变量效应;(ii)修改协变量表示方法;(iii)引入相关儿科协变量效应(年龄对时间依赖性清除的衰减系数和 ALL 效应(疾病类型和/或不同的生物分析方法)对时间依赖性清除的初始值)。对于复发/难治性 BCP-ALL 患者,年龄增加与时间依赖性清除的衰减系数降低相关,表明儿童的靶向介导药物清除速度更快。在儿科 BCP-ALL 患者中,第 1 个周期结束时,缓解者(n=42)的累积浓度-时间曲线下面积中位数(四分位距)显著高于未缓解者(n=10)(26.1[18.9-35.0]比 10.1[9.19-16.1]×10ng*h/mL,p<0.001)。在推荐的儿科 II 期剂量的模拟中,依妥珠单抗奥佐米星的暴露量达到了在儿科试验参与者中观察到的相似水平。
本研究中,依妥珠单抗奥佐米星在复发/难治性 BCP-ALL 儿科患者中的药代动力学特征得到了很好的描述。基于推荐的儿科 II 期剂量的依妥珠单抗奥佐米星暴露量模拟,对于儿科 BCP-ALL 患者,无需进行临床剂量调整,即可获得预期的疗效和可接受的耐受性。