Department of Anesthesiology and Critical Care Medicine, School of Medicine, Fujita Health University, 1-98 Dengakugakubo, Kutsukake-cho, Toyoake, Aichi, 470-1192, Japan.
Department of Cardiovascular Surgery, School of Medicine, Fujita Health University, Toyoake, Aichi, Japan.
J Cardiothorac Surg. 2024 Jun 24;19(1):358. doi: 10.1186/s13019-024-02890-w.
Infective endocarditis (IE) is a rare cardiovascular complication in patients with coronavirus disease 2019 (COVID-19). IE after COVID-19 can also be complicated by acute respiratory distress syndrome (ARDS); however, the guidelines for the treatment of such cases are not clear. Here, we report a case of perioperative management of post-COVID-19 IE with ARDS using veno-venous extracorporeal membrane oxygenation (V-V ECMO).
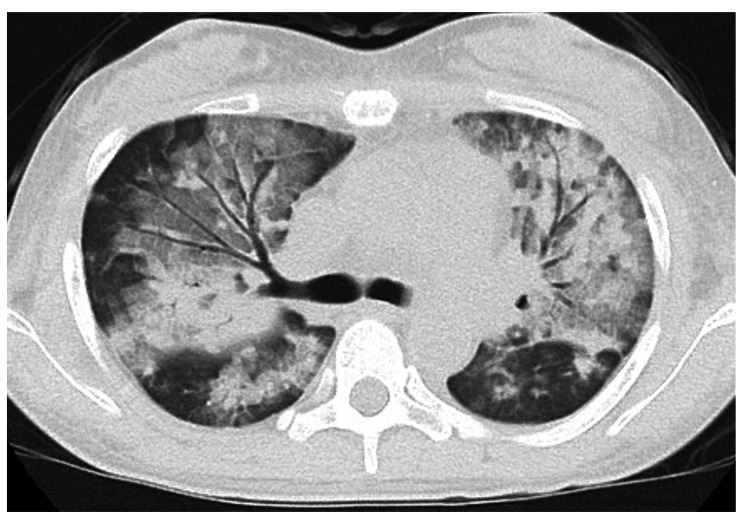
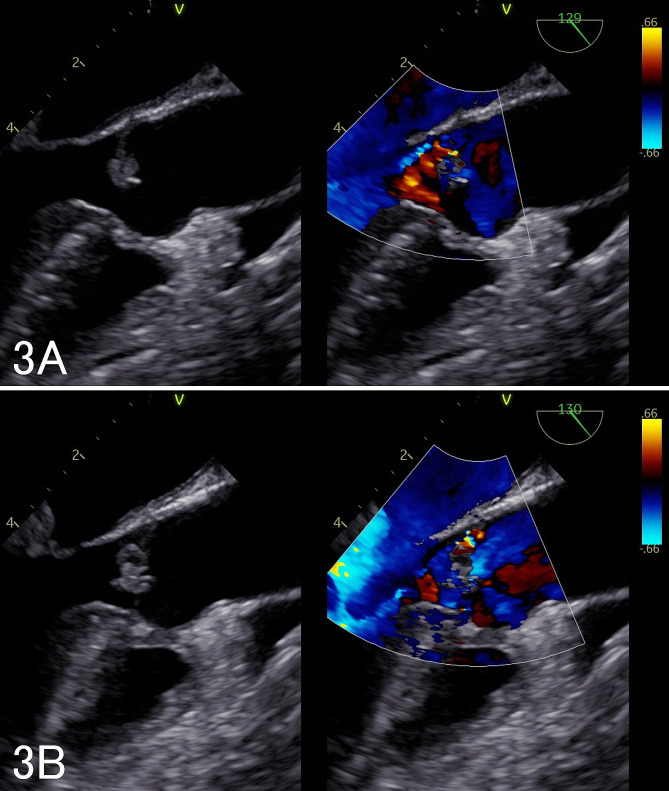
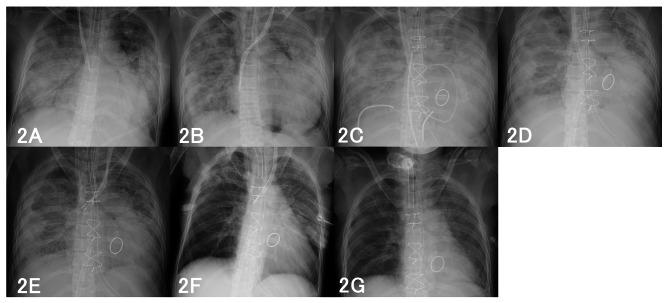
The patient was a 40-year-old woman who was admitted on day 18 of COVID-19 onset and was administered oxygen therapy, remdesivir, and dexamethasone. The patient's condition improved; however, on day 24 of hospitalization, the patient developed hypoxemia and was admitted to the intensive care unit (ICU) due to respiratory failure. Blood culture revealed Corynebacterium striatum, and transesophageal echocardiography revealed vegetation on the aortic and mitral valves. Valve destruction was mild, and the cause of respiratory failure was thought to be ARDS. Despite continued antimicrobial therapy, ARDS did not improve the patient's condition, and valve destruction progressed; therefore, surgical treatment was scheduled on day 13 of ICU admission. After preoperative consultation with the team, a decision was made to initiate V-V ECMO after the patient was weaned from CPB, with concerns about further worsening of her respiratory status after surgery. The patient returned to the ICU with transition to V-V ECMO, and her circulation remained stable. The patient was weaned off V-V ECMO on postoperative day 33 and discharged from the ICU on postoperative day 47.
ARDS may occur in patients with IE after COVID-19. Owing to concerns about further exacerbation of pulmonary damage, the timing of surgery should be comprehensively considered. Preoperatively, clinicians should discuss perioperative ECMO introduction and configuration.
感染性心内膜炎(IE)是 2019 年冠状病毒病(COVID-19)患者罕见的心血管并发症。COVID-19 后发生的 IE 也可并发急性呼吸窘迫综合征(ARDS);然而,此类病例的治疗指南并不明确。在此,我们报告了一例使用静脉-静脉体外膜肺氧合(V-V ECMO)治疗 COVID-19 后 IE 合并 ARDS 的围手术期管理病例。
患者为 40 岁女性,COVID-19 发病第 18 天入院,给予氧疗、瑞德西韦和地塞米松治疗。患者病情改善;然而,住院第 24 天,患者出现低氧血症,并因呼吸衰竭转入重症监护病房(ICU)。血培养显示 Corynebacterium striatum,经食管超声心动图显示主动脉瓣和二尖瓣有赘生物。瓣膜破坏轻微,呼吸衰竭的原因被认为是 ARDS。尽管继续进行抗菌治疗,ARDS 仍未改善患者的病情,且瓣膜破坏进展;因此,在 ICU 入院第 13 天安排了手术治疗。在与团队进行术前咨询后,决定在患者从体外循环脱机后启动 V-V ECMO,担心手术后其呼吸状况进一步恶化。患者带着 V-V ECMO 回到 ICU,循环保持稳定。患者在术后第 33 天成功脱机 V-V ECMO,并在术后第 47 天从 ICU 出院。
COVID-19 后发生的 IE 可能并发 ARDS。由于担心肺部损伤进一步加重,手术时机应综合考虑。术前,临床医生应讨论围手术期 ECMO 的引入和配置。