The Donald and Barbara Zucker School of Medicine and Hofstra/Northwell, The Feinstein Institute for Medical Research, and Department of Medicine, Anticoagulation and Clinical Thrombosis Services Northwell Health at Lenox Hill Hospital, New York, New York.
Department of Medicine and Surgery, University of Insubria, Varese, Italy.
J Am Coll Cardiol. 2020 Jun 30;75(25):3140-3147. doi: 10.1016/j.jacc.2020.04.071.
Hospitalized acutely ill medical patients are at risk for fatal and major thromboembolic events. Whether use of extended-duration primary thromboprophylaxis can prevent such events is unknown.
The purpose of this study was to evaluate whether extended-duration rivaroxaban reduces the risk of venous and arterial fatal and major thromboembolic events without significantly increasing major bleeding in acutely ill medical patients after discharge.
MARINER (A Study of Rivaroxaban [JNJ-39039039] on the Venous Thromboembolic Risk in Post-Hospital Discharge Patients) studied acutely ill medical patients with additional risk factors for venous thromboembolism (VTE). Medically ill patients with a baseline creatinine clearance ≥50 ml/min were randomized in a double-blind fashion to rivaroxaban 10 mg or placebo daily at hospital discharge for 45 days. Exploratory efficacy analyses were performed with the intent-to-treat population including all data through day 45. Time-to-event curves were calculated using the Kaplan-Meier method. A blinded independent committee adjudicated all clinical events.
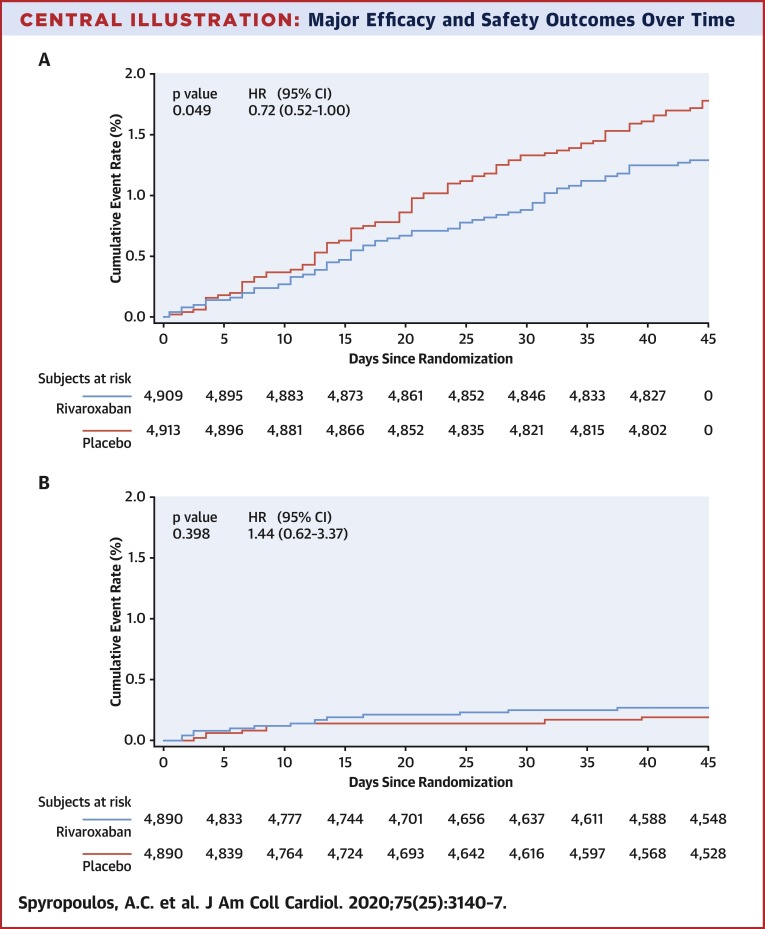
In total, 4,909 patients were assigned to rivaroxaban and 4,913 patients to placebo. The mean age was 67.8 years, 55.5% were men, mean baseline creatinine clearance was 87.8 ml/min, and mean duration of hospitalization was 6.7 days. The pre-specified composite efficacy endpoint (symptomatic VTE, myocardial infarction, nonhemorrhagic stroke, and cardiovascular death) occurred in 1.28% and 1.77% of patients in the rivaroxaban and placebo groups, respectively (hazard ratio: 0.72; 95% confidence interval: 0.52 to 1.00; p = 0.049), whereas major bleeding occurred in 0.27% and 0.18% of patients in the rivaroxaban and placebo groups, respectively (hazard ratio: 1.44; 95% confidence interval: 0.62 to 3.37; p = 0.398).
Extended-duration rivaroxaban in hospitalized medically ill patients resulted in a 28% reduction in fatal and major thromboembolic events without a significant increase in major bleeding. (A Study of Rivaroxaban [JNJ-39039039] on the Venous Thromboembolic Risk in Post-Hospital Discharge Patients [MARINER]; NCT02111564).
住院急性病患者有发生致命性和主要血栓栓塞事件的风险。使用延长疗程的初级血栓预防是否可以预防此类事件尚不清楚。
本研究旨在评估延长疗程的利伐沙班是否可以降低出院后急性病住院患者静脉和动脉致命性和主要血栓栓塞事件的风险,同时不显著增加大出血。
MARINER(利伐沙班[JNJ-39039039]对出院后患者静脉血栓栓塞风险的研究)研究了伴有静脉血栓栓塞(VTE)额外风险因素的急性病住院患者。基线肌酐清除率≥50ml/min的住院患者以双盲方式随机分为利伐沙班 10mg 或安慰剂,每天一次,在出院后 45 天内使用。通过意向治疗人群进行探索性疗效分析,该人群包括所有数据至第 45 天。使用 Kaplan-Meier 方法计算时间-事件曲线。一个盲法独立委员会对所有临床事件进行了裁决。
共有 4909 名患者被分配至利伐沙班组,4913 名患者被分配至安慰剂组。患者平均年龄为 67.8 岁,55.5%为男性,平均基线肌酐清除率为 87.8ml/min,平均住院时间为 6.7 天。预定的复合疗效终点(有症状的 VTE、心肌梗死、非出血性卒中和心血管死亡)在利伐沙班组和安慰剂组中的发生率分别为 1.28%和 1.77%(风险比:0.72;95%置信区间:0.52 至 1.00;p=0.049),而大出血在利伐沙班组和安慰剂组中的发生率分别为 0.27%和 0.18%(风险比:1.44;95%置信区间:0.62 至 3.37;p=0.398)。
在住院的有疾病的患者中,延长疗程的利伐沙班可使致命性和主要血栓栓塞事件减少 28%,而大出血发生率无显著增加。(利伐沙班[JNJ-39039039]对出院后患者静脉血栓栓塞风险的研究[MARINER];NCT02111564)。