Department of Laboratory Medicine & Pathology, University of Washington, Seattle, WA, United States of America.
Department of Radiation-Oncology, Washington University School of Medicine, St. Louis, MO, United States of America.
Exp Mol Pathol. 2024 Aug;138:104915. doi: 10.1016/j.yexmp.2024.104915. Epub 2024 Jul 3.
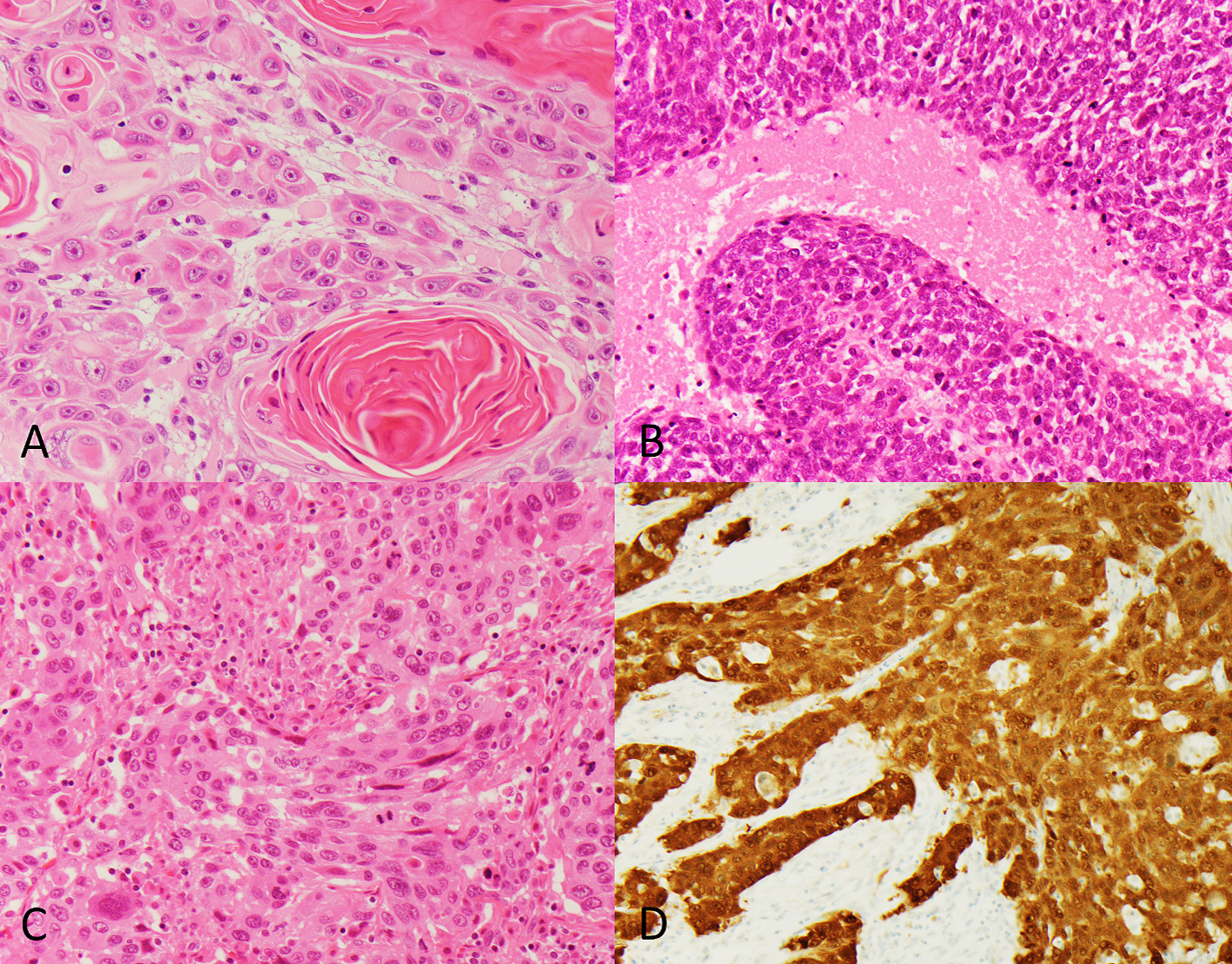
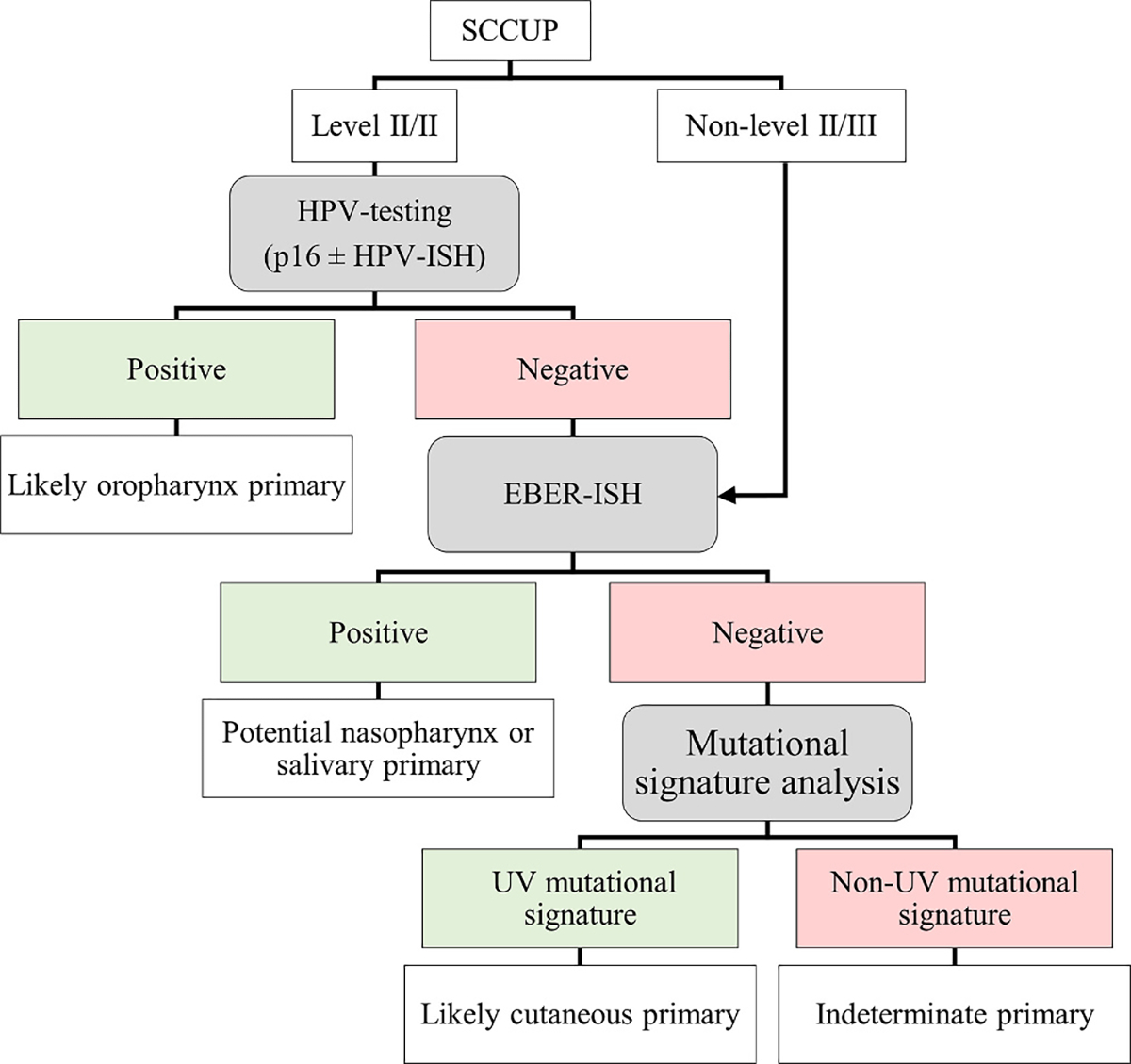
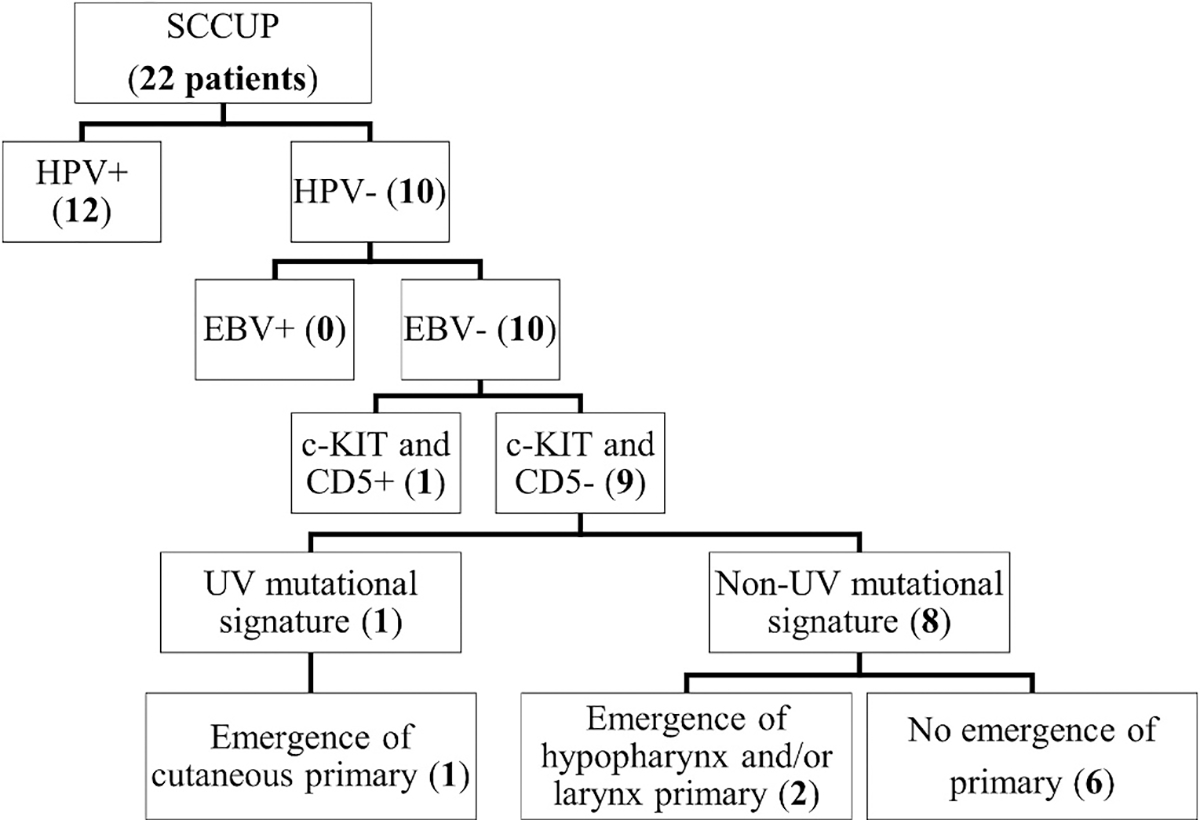
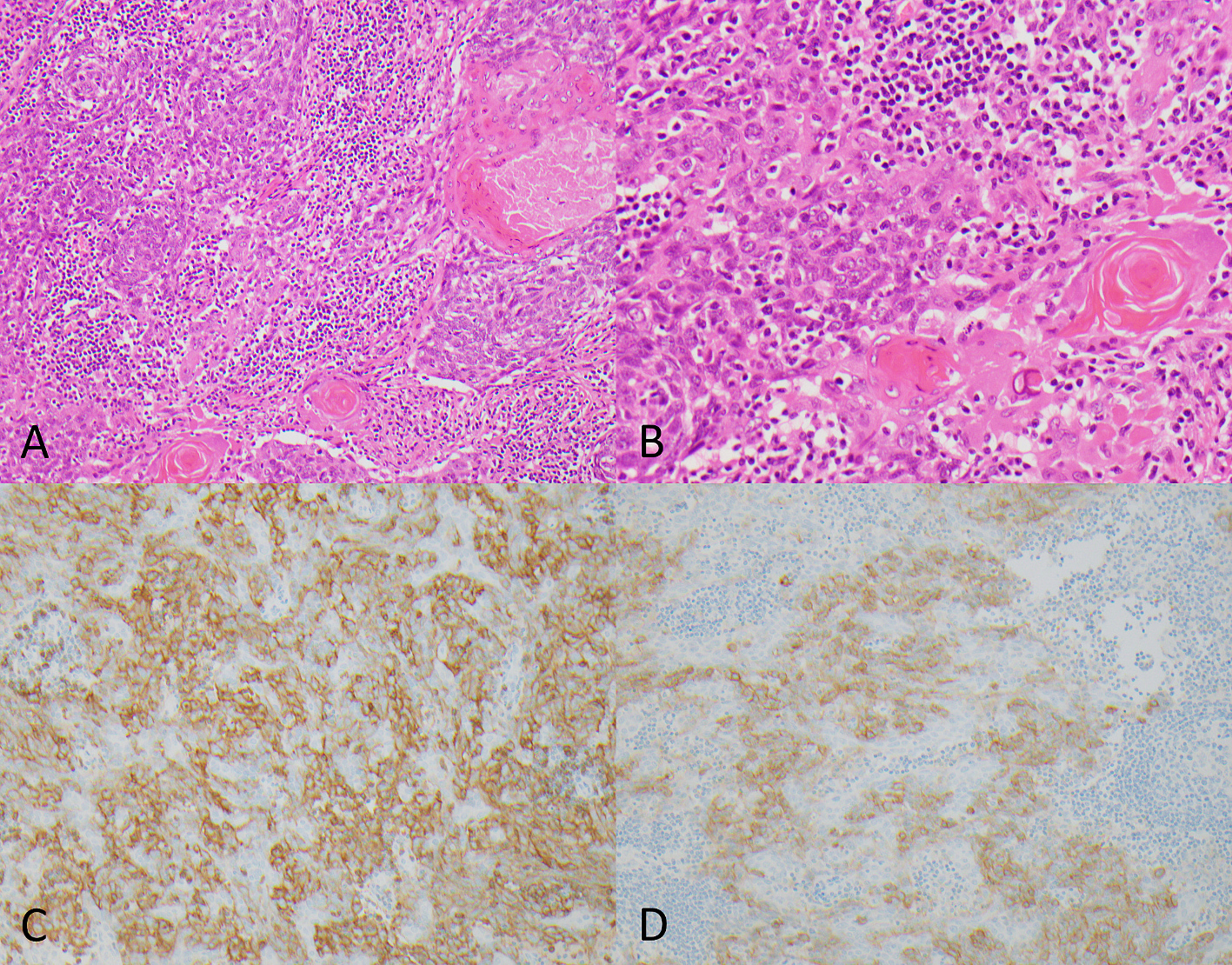
A subset of head and neck squamous cell carcinomas present solely as metastatic disease in the neck and are of unknown primary origin (SCCUP). Most primary tumors will ultimately be identified, usually in the oropharynx. In a minority of cases, the primary site remains elusive. Here, we examine the role of ancillary testing, including mutational signature analysis (MSA), to help identify likely primary sites in such cases. Twenty-two cases of SCCUP in the neck, collected over a 10-year period, were classified by morphology and viral status; including human papillomavirus (HPV) testing by p16 immunohistochemistry (IHC) and RT-qPCR, as well as Epstein-Barr virus (EBV) testing by EBER-ISH. CD5 and c-KIT (CD117) IHC was done to evaluate for possible thymic origin in all virus-negative cases. Whole exome sequencing, followed by MSA, was used to identify UV signature mutations indicative of cutaneous origin. HPV was identified in 12 of 22 tumors (54.5%), favoring an oropharyngeal origin, and closely associated with nonkeratinizing tumor morphology (Fisher's exact test; p = 0.0002). One tumor with indeterminant morphology had discordant HPV and p16 status (p16+/HPV-). All tumors were EBV-negative. Diffuse expression of CD5 and c-KIT was identified in 1 of 10 virus-negative SCCUPs (10%), suggesting a possible ectopic thymic origin rather than a metastasis. A UV mutational signature, indicating cutaneous origin, was identified in 1 of 10 (10%) virus-negative SCCUPs. A cutaneous auricular primary emerged 3 months after treatment in this patient. Primary tumors became clinically apparent in 2 others (1 hypopharynx, 1 hypopharynx/larynx). Thus, after follow-up, 6 tumors remained unclassifiable as to the possible site of origin (27%). Most SCCUPs of the neck in our series were HPV-associated and thus likely of oropharyngeal origin. UV signature mutation analysis and additional IHC for CD5 and c-KIT for possible thymic origin may aid in further classifying virus-negative unknown primaries. Close clinical inspection of hypopharyngeal mucosa may also be helpful, as a subset of primary tumors later emerged at this site.
一组头颈部鳞状细胞癌仅表现为颈部转移性疾病,且原发灶不明(SCCUP)。大多数原发肿瘤最终会被确定,通常是在口咽。在少数情况下,原发灶仍然难以确定。在这里,我们研究了辅助检测的作用,包括突变特征分析(MSA),以帮助确定此类病例中可能的原发部位。收集了过去 10 年中颈部的 22 例 SCCUP,通过形态学和病毒状态进行分类;包括人乳头瘤病毒(HPV)检测,通过 p16 免疫组化(IHC)和 RT-qPCR,以及 Epstein-Barr 病毒(EBV)检测,通过 EBER-ISH。对所有病毒阴性病例进行 CD5 和 c-KIT(CD117)免疫组化以评估可能的胸腺起源。全外显子组测序,随后是 MSA,用于鉴定表明皮肤起源的 UV 特征突变。在 22 个肿瘤中有 12 个(54.5%)检测到 HPV,提示口咽起源,并与非角化肿瘤形态密切相关(Fisher 精确检验;p=0.0002)。一个形态学不确定的肿瘤具有不一致的 HPV 和 p16 状态(p16+/HPV-)。所有肿瘤均为 EBV 阴性。10 例病毒阴性 SCCUP 中有 1 例(10%)弥漫表达 CD5 和 c-KIT,提示可能为异位胸腺起源而不是转移。10 例病毒阴性 SCCUP 中有 1 例(10%)鉴定出 UV 突变特征,提示皮肤起源。在该患者中,治疗后 3 个月出现了皮肤耳廓原发性肿瘤。在另外 2 例中(1 例下咽,1 例下咽/喉),原发肿瘤变得明显。因此,经过随访,6 个肿瘤仍然无法确定可能的起源部位(27%)。我们系列中的大多数颈部 SCCUP 与 HPV 相关,因此可能来源于口咽。UV 特征突变分析和 CD5 和 c-KIT 的额外 IHC 可能有助于进一步分类病毒阴性的未知原发灶。密切观察下咽黏膜的临床情况也可能有所帮助,因为一组原发性肿瘤随后在此部位出现。