Department of Medicine, Hackensack University Medical Center, Hackensack, NJ, USA.
Department of Pulmonary and Critical Care, Hackensack University Medical Center, Hackensack, NJ, USA.
Am J Case Rep. 2024 Jul 6;25:e943740. doi: 10.12659/AJCR.943740.
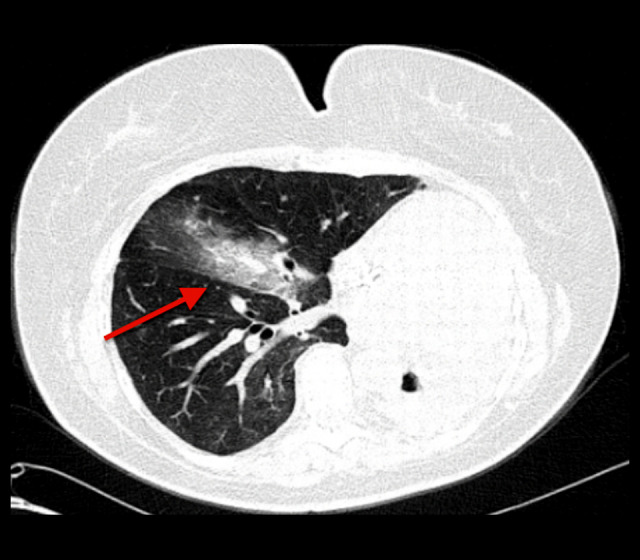
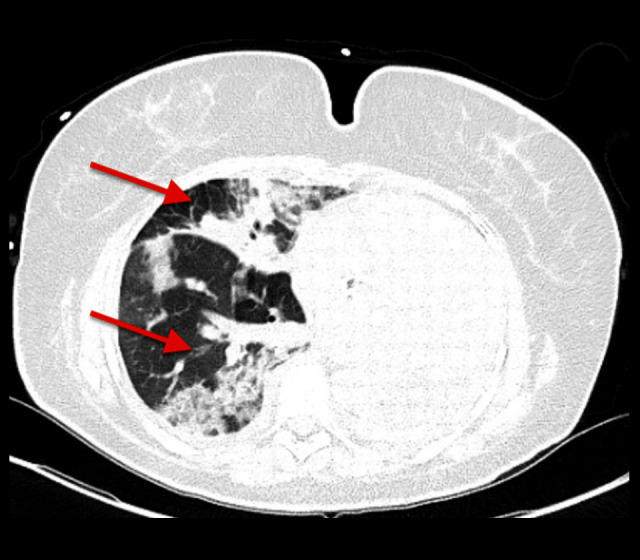
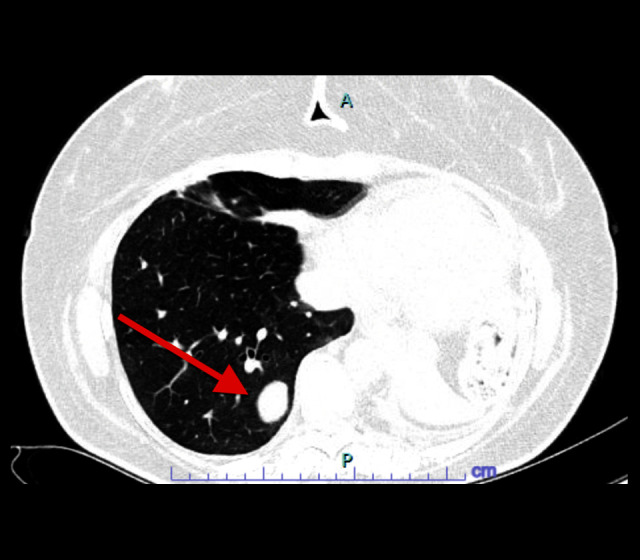
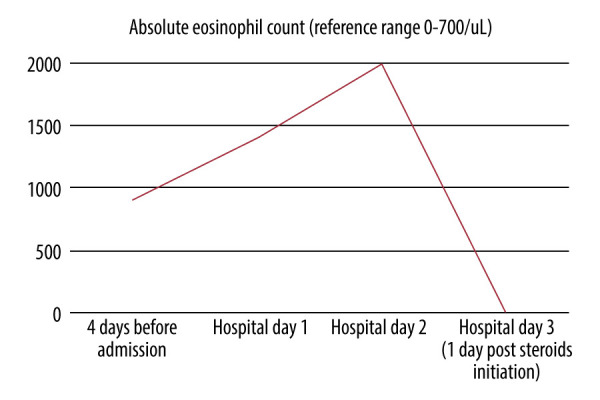
BACKGROUND Immune checkpoint inhibitors (ICIs) have been linked to various immune-related adverse events, including pneumonitis, necessitating early recognition and potential treatment discontinuation. Acute eosinophilic pneumonia (AEP) induced by ICIs, particularly with no reported cases involving anti-TIGIT therapy, is rare. This report describes a case of AEP following treatment with pembrolizumab and anti-TIGIT therapy. CASE REPORT A 46-year-old woman with lung adenoid cystic carcinoma and chronic hypoxemic respiratory failure on long-term oxygen therapy presented with fever, cough, and shortness of breath. She underwent left pneumonectomy and radiation therapy at diagnosis 9 years earlier. She was participating in a clinical trial using pembrolizumab and anti-TIGIT EOS-448, due to cancer progression. After starting therapy, she developed stable peripheral eosinophilia and a skin rash, suggestive of a drug reaction. On admission, she was in acute-on-chronic hypoxemic respiratory failure, febrile, with an elevated eosinophil count and new multifocal infiltrates in the right lung. Despite broad antibiotics coverage for pneumonia, she developed worsening respiratory symptoms and eosinophilia. She was then empirically started on intravenous methylprednisolone for acute eosinophilic pneumonia without confirmatory bronchoscopy as she was at high risk with her previous pneumonectomy. She subsequently had rapid improvement in her symptoms. CONCLUSIONS AEP should be considered in patients treated with ICIs who develop immune-related adverse effects. Although bronchoscopy findings are part of AEP's diagnostic criteria, this case underscores the importance of clinical judgment in the prompt initiation of steroids, even without confirmatory bronchoscopy, in rapidly progressing cases. The role of anti-TIGIT therapy in this context remains uncertain.
免疫检查点抑制剂(ICIs)与各种免疫相关不良反应相关,包括肺炎,需要早期识别并可能停止治疗。ICI 引起的急性嗜酸性肺炎(AEP),特别是没有报告涉及抗 TIGIT 治疗的病例,较为罕见。本报告描述了一例使用 pembrolizumab 和抗 TIGIT 治疗后发生 AEP 的病例。
一名 46 岁女性,患有肺腺样囊性癌,长期氧疗导致慢性低氧性呼吸衰竭,因发热、咳嗽和呼吸急促就诊。9 年前她被诊断出患有肺腺癌,行左肺切除术和放射治疗。她正在参与一项使用 pembrolizumab 和抗 TIGIT EOS-448 的临床试验,因为癌症进展。开始治疗后,她出现稳定的外周血嗜酸性粒细胞增多和皮疹,提示药物反应。入院时,她处于慢性低氧性呼吸衰竭急性加重期,发热,嗜酸性粒细胞计数升高,右肺新发多灶性浸润。尽管广谱抗生素覆盖了肺炎,但她的呼吸症状和嗜酸性粒细胞增多仍在恶化。由于她之前的肺切除术风险较高,她未经支气管镜确诊就经验性地开始静脉注射甲基强的松龙治疗急性嗜酸性肺炎。随后她的症状迅速改善。
接受 ICI 治疗并出现免疫相关不良反应的患者应考虑 AEP。虽然支气管镜检查结果是 AEP 诊断标准的一部分,但本病例强调了在快速进展的病例中,即使没有支气管镜确诊,根据临床判断迅速开始使用类固醇的重要性。抗 TIGIT 治疗在这种情况下的作用仍不确定。