Bruckner Howard W, De Jager Robert, Knopf Elisheva, Bassali Fred, Book Abe, Gurell Daniel, Nghiem Van, Schwartz Myron, Hirschfeld Azriel
Department of Oncology, MZB Foundation for Cancer Research, New York, NY, United States.
Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, United States.
Front Oncol. 2024 Jun 24;14:1361420. doi: 10.3389/fonc.2024.1361420. eCollection 2024.
Routine blood tests are prognostic tests for patients with cholangiocarcinoma. New drug regimens may produce a median overall survival of 2 years or more.
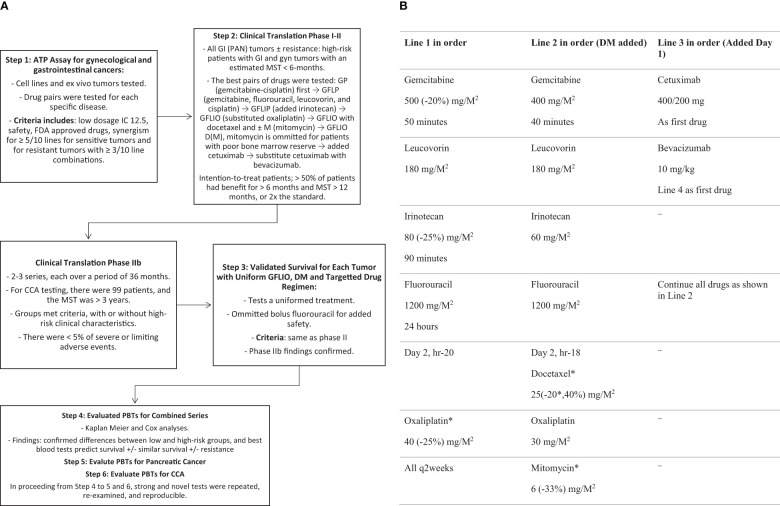
This single practice, IRB-approved, phase II trial examines prognostic tests, Kaplan-Meier survival, and univariate Cox regression analyses. Eligibility requires: intent-to-treat; signed consent; advanced measurable intrahepatic cholangiocarcinoma, with or without resistance to the test drugs; any adult age; performance status 0-2; and expected survival of ≥ 6 weeks. Biweekly treatment, with 1/3 of standard dosages in mg/M, includes: Gemcitabine 500; 5-Fluorouracil 1200 over 24 hours; Leucovorin 180; Irinotecan 80; and on day 2, Oxaliplatin 40. On progression, drugs are added on day 2: first, Docetaxel 25 precedes Oxaliplatin, with or without Mitomycin C 6 after Oxaliplatin. The next sequential additions are day 1, Cetuximab 400 total mg, then 200 mg weekly, and then Bevacizumab 10 mg/kg is substituted for Cetuximab (FDA IND# 119005).
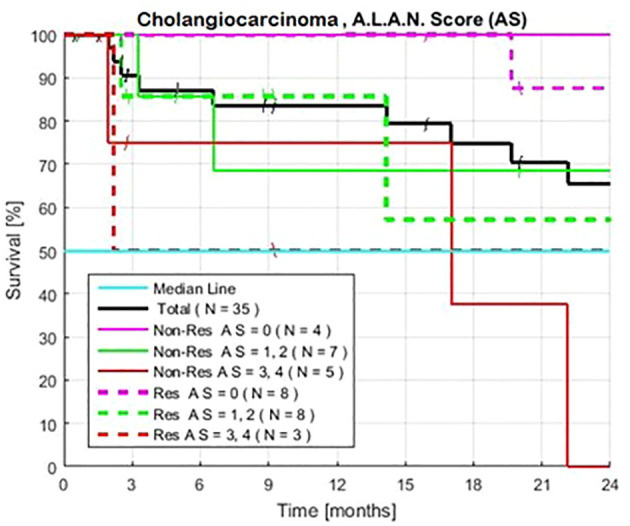
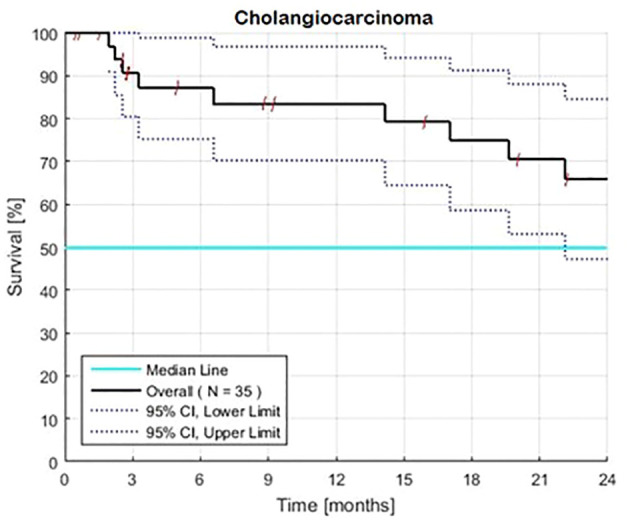
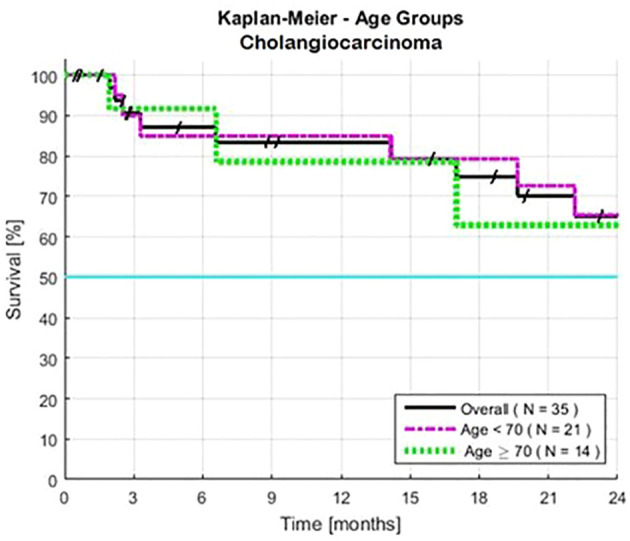
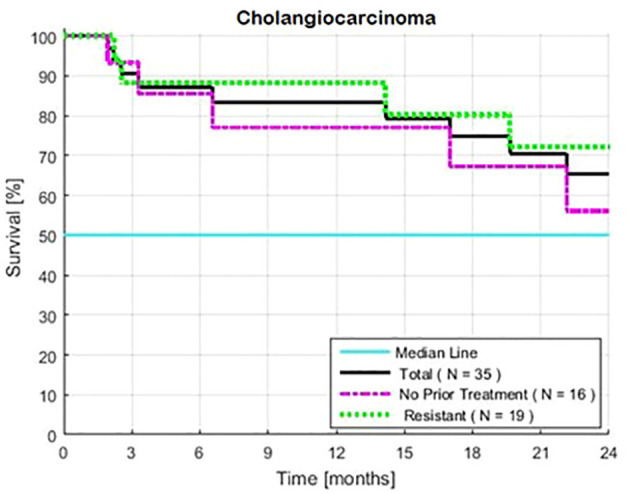
For 35 patients, 19 with 1-2 lines of prior therapy, resistant tumors, and 16 no prior therapy, survival at 24-months is ≥ 72 and ≥ 58%, respectively. For 14 patients aged ≥ 70 years, ≥ 63% survive 24 months, P = 0.28. Validated tests that predict ≤ 6-month survivals find median survival times of 17-months through > 2-years when compared to patients with favorable tests: Neutrophils lymphocyte ratio > 3.0, HR = 6.54, P < 6.4x10-3; absolute neutrophil count > 8000/μl, HR = 4.95, P < 6.5x10-3; serum albumin < 3.5 g/dl, HR = 4.10, P < 0.03; and lymphocyte monocyte ratio< 2.1, HR = 1.6, P = 0.50. Overall, the 76 (60-90)% of patients with 0-2 out of 4 high risk tests survive ≥ 24 months, (P = 7.1x10-3). Treatments produce neither hospitalization, neutropenic fever, severe enteritis, nor severe neuropathies.
Two-year survival is replicable and predictable. Findings warrant phase III validation tests of sequential regimens, re-challenge with recombination, low dosages, and blood tests that are associated with lethal mechanisms that impair response and survival.
常规血液检查对胆管癌患者具有预后评估作用。新的药物方案可能使中位总生存期达到2年或更长。
本单中心、经机构审查委员会(IRB)批准的II期试验对预后检查、Kaplan-Meier生存分析和单变量Cox回归分析进行了研究。入选标准包括:意向性治疗;签署知情同意书;晚期可测量的肝内胆管癌,无论对试验药物有无耐药性;任何成年年龄;体能状态为0 - 2;预期生存期≥6周。每两周进行一次治疗,剂量为标准剂量的1/3(mg/M),包括:吉西他滨500;5-氟尿嘧啶1200,在24小时内输注;亚叶酸钙180;伊立替康80;在第2天,奥沙利铂40。病情进展时,在第2天添加药物:首先,多西他赛25在奥沙利铂之前使用,奥沙利铂之后可加或不加丝裂霉素C 6。接下来依次添加的药物为:第1天,西妥昔单抗总剂量400mg,然后每周200mg,然后用贝伐单抗10mg/kg替代西妥昔单抗(FDA IND# 119005)。
35例患者中,19例接受过1 - 2线先前治疗且肿瘤耐药,16例未接受过先前治疗,24个月时的生存率分别≥72%和≥58%。14例年龄≥70岁的患者中,≥63%存活24个月,P = 0.28。经验证可预测生存期≤6个月的检查发现,与检查结果良好的患者相比,中位生存时间为17个月至超过2年:中性粒细胞与淋巴细胞比值>3.0,HR = 6.54,P < 6.4×10⁻³;绝对中性粒细胞计数>8000/μl,HR = 4.95,P < 6.5×10⁻³;血清白蛋白<3.5g/dl,HR = 4.10,P < 0.03;淋巴细胞与单核细胞比值<2.1,HR = 1.6,P = 0.50。总体而言,4项高风险检查中0 - 2项为高风险的患者中,76(60 - 90)%存活≥24个月,(P = 7.1×10⁻³)。治疗未导致住院、中性粒细胞减少性发热、严重肠炎或严重神经病变。
两年生存率具有可重复性和可预测性。研究结果值得对序贯方案进行III期验证试验,采用重组、低剂量以及与损害反应和生存的致死机制相关的血液检查进行再挑战。