Foca Marc, Demirhan Salih, Munoz Flor M, Valencia Deray Kristen G, Bocchini Claire E, Sharma Tanvi S, Sherman Gilad, Muller William J, Heald-Sargent Taylor, Danziger-Isakov Lara, Blum Samantha, Boguniewicz Juri, Bacon Samantha, Joseph Tuhina, Smith Jodi, Ardura Monica I, Su Yin, Maron Gabriela M, Ferrolino Jose, Herold Betsy C
Division of Infectious Diseases, Department of Pediatrics, Children's Hospital at Montefiore, Albert Einstein College of Medicine, Bronx, New York, USA.
Division of Infectious Diseases, Department of Pediatrics, Texas Children's Hospital, Baylor College of Medicine, Houston, Texas, USA.
Open Forum Infect Dis. 2024 Jul 1;11(7):ofae353. doi: 10.1093/ofid/ofae353. eCollection 2024 Jul.
Valganciclovir is the only approved antiviral for cytomegalovirus (CMV) prevention in pediatric solid organ transplantation (SOT). Additional approaches may be needed to improve outcomes.
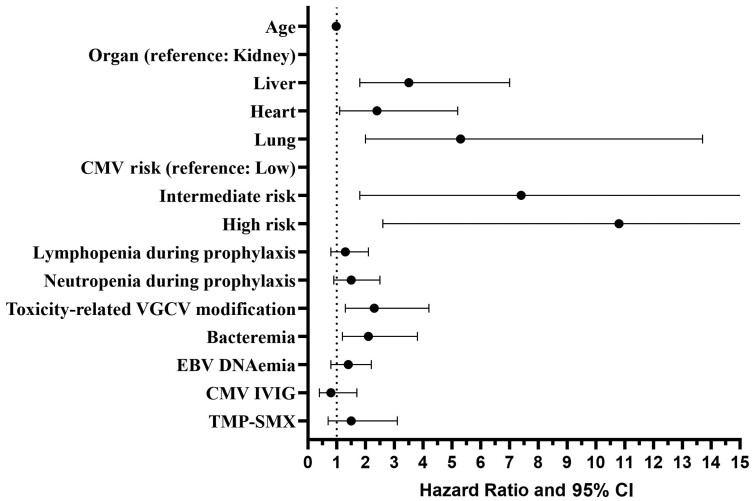
A multicenter retrospective study from 2016 to 2019 was conducted of pediatric SOT recipients in whom at least 3 months of valganciclovir prophylaxis was planned. Episodes of CMV DNA in blood (DNAemia), CMV disease, drug-related toxicities, as well as other infections in the first year posttransplant and demographic and clinical data were collected. CMV DNAemia in the first year after prophylaxis or during prophylaxis (breakthrough) was analyzed by multivariate hazard models.
Among the 749 patients enrolled, 131 (17.5%) had CMV DNAemia at any time in the first year; 85 (11.4%) had breakthrough DNAemia, and 46 (6.1%) had DNAemia after prophylaxis. CMV disease occurred in 30 (4%). In a multivariate model, liver transplantation compared to kidney or heart, intermediate or high risk based on donor/recipient serologies, neutropenia, and valganciclovir dose modifications attributed to toxicity were associated with increased risk of total and/or breakthrough DNAemia. Bacteremia was also associated with increased hazard ratio for CMV DNAemia. In a separate multivariate analysis, rejection occurred more often in those with breakthrough CMV DNAemia ( = .002); liver transplants, specifically, had increased rejection if CMV DNAemia occurred in the first year ( = .004). These associations may be bidirectional as rejection may contribute to infection risk.
CMV DNAemia in the first year posttransplantation occurs despite valganciclovir prophylaxis and is associated with medication toxicity, bacteremia, and rejection. Pediatric studies of newer antivirals, especially in higher-risk subpopulations, appear to be warranted.
缬更昔洛韦是儿科实体器官移植(SOT)中唯一获批用于预防巨细胞病毒(CMV)的抗病毒药物。可能需要其他方法来改善治疗效果。
对2016年至2019年计划接受至少3个月缬更昔洛韦预防治疗的儿科SOT受者进行了一项多中心回顾性研究。收集移植后第一年血液中CMV DNA(DNA血症)、CMV疾病、药物相关毒性以及其他感染情况,以及人口统计学和临床数据。通过多变量风险模型分析预防后或预防期间(突破性)第一年的CMV DNA血症。
在纳入的749例患者中,131例(17.5%)在第一年的任何时间出现CMV DNA血症;85例(11.4%)出现突破性DNA血症,46例(6.1%)在预防后出现DNA血症。30例(4%)发生CMV疾病。在多变量模型中,与肾移植或心脏移植相比,肝移植、基于供体/受体血清学的中或高风险、中性粒细胞减少以及因毒性导致的缬更昔洛韦剂量调整与总DNA血症和/或突破性DNA血症风险增加相关。菌血症也与CMV DNA血症的风险比增加相关。在另一项多变量分析中,突破性CMV DNA血症患者发生排斥反应的频率更高(P = 0.002);具体而言,如果肝移植患者在第一年出现CMV DNA血症,则排斥反应增加(P = 0.004)。这些关联可能是双向的,因为排斥反应可能会增加感染风险。
尽管使用了缬更昔洛韦预防,移植后第一年仍会出现CMV DNA血症,且与药物毒性、菌血症和排斥反应相关。似乎有必要对新型抗病毒药物进行儿科研究,尤其是在高风险亚人群中。