Department of Cardiology, University and Hospital Fribourg, Fribourg, Switzerland.
Tex Heart Inst J. 2024 Jul 10;51(2). doi: 10.14503/THIJ-23-8267.
Various scoring systems have been developed to assess the risk of bleeding in medical settings. HAS-BLED and HEMORR2HAGES risk scores are commonly used to estimate bleeding risk in patients receiving anticoagulation for atrial fibrillation, but data on their predictive value in patients undergoing percutaneous coronary intervention (PCI) are limited.
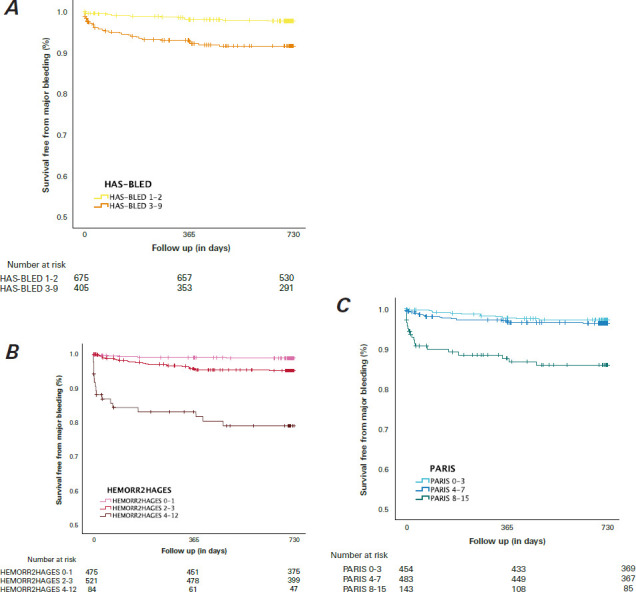
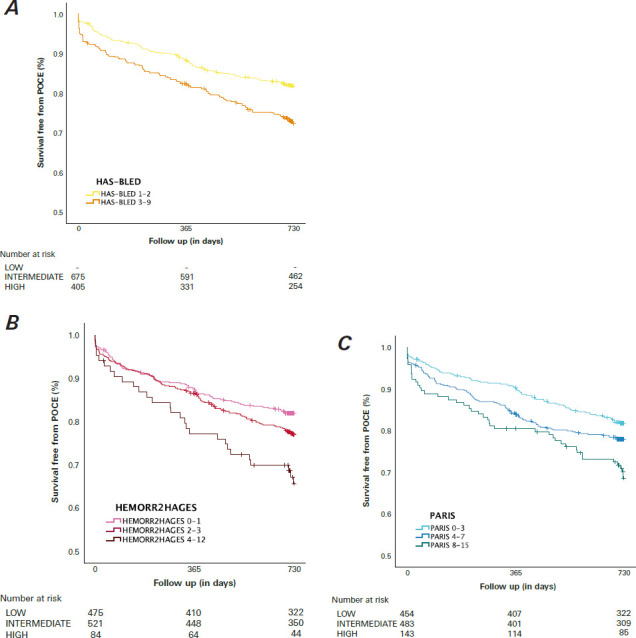
This study evaluated and compared the predictive abilities of the HAS-BLED and HEMORR2HAGES bleeding risk scores in all-comer patients undergoing PCI. The PARIS score, specifically designed for patients undergoing PCI, was used as a comparator. The scores were calculated at baseline and compared with the occurrence of events during a 2-year clinical follow-up period. Between 2015 and 2017, all consecutive patients undergoing PCI we re prospectively enrolled and divided into risk tertiles based on bleeding risk scores. The primary end points were hierarchical major bleeding events, defined by Bleeding Academic Research Consortium types 3 through 5, and patient-oriented composite end points according to Bleeding Academic Research Consortium classification, which were assessed during the 2-year follow-up period.
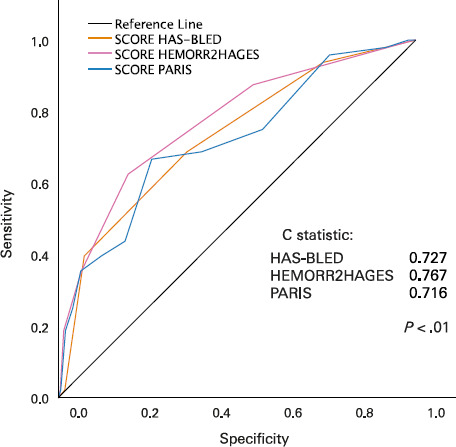
A total of 1,080 patients completed the follow-up period. Two years after index, 189 patients (17.5%) had experienced any bleeding, with 48 events (4.4%) classified as Bleeding Academic Research Consortium types 3 to 5. All bleeding risk scores showed statistically significant predictive ability for bleeding events. The HEMORR2HAGES score (C statistic, 0.73) was more effective than the HAS-BLED score (C statistic, 0.66; P = .07) and the PARIS score (C statistic, 0.66; P = .06) in predicting risk of major bleeding. Patients in high-risk bleeding groups also experienced a higher incidence of patient-oriented composite end points.
The HEMORR2HAGES, HAS-BLED, and PARIS risk scores exhibited good predictive abilities for bleeding events following PCI. Patients at high risk of bleeding also demonstrated increased ischemic risk and higher mortality during the 2-year follow-up period.
已经开发出各种评分系统来评估医疗环境中的出血风险。HAS-BLED 和 HEMORR2HAGES 风险评分常用于评估接受心房颤动抗凝治疗的患者的出血风险,但关于这些评分在接受经皮冠状动脉介入治疗(PCI)的患者中的预测价值的数据有限。
本研究评估并比较了 HAS-BLED 和 HEMORR2HAGES 出血风险评分在所有接受 PCI 的患者中的预测能力。专门为接受 PCI 的患者设计的 PARIS 评分被用作对照。在 2 年临床随访期间,根据基线时的评分与事件发生情况进行比较。在 2015 年至 2017 年期间,所有连续接受 PCI 的患者均前瞻性入组,并根据出血风险评分分为风险三分位组。主要终点是由 Bleeding Academic Research Consortium 类型 3 至 5 定义的分层主要出血事件,以及根据 Bleeding Academic Research Consortium 分类评估的患者导向复合终点,在 2 年随访期间进行评估。
共有 1080 例患者完成了随访。指数后 2 年,189 例患者(17.5%)发生任何出血,其中 48 例事件(4.4%)被归类为 Bleeding Academic Research Consortium 类型 3 至 5。所有出血风险评分均显示出对出血事件具有统计学意义的预测能力。HEMORR2HAGES 评分(C 统计量,0.73)比 HAS-BLED 评分(C 统计量,0.66;P =.07)和 PARIS 评分(C 统计量,0.66;P =.06)更有效地预测主要出血风险。高出血风险组的患者也经历了更高的患者导向复合终点发生率。
HEMORR2HAGES、HAS-BLED 和 PARIS 风险评分对 PCI 后出血事件具有良好的预测能力。在 2 年随访期间,高出血风险的患者也表现出增加的缺血风险和更高的死亡率。