Department of Health and Caring Sciences, Faculty of Health and Life Sciences, Linnaeus University, 39182, Kalmar, Sweden.
Department of Pharmacy, Faculty of Health Sciences, UiT The Arctic University of Norway, Tromsø, Norway.
BMC Geriatr. 2024 Jul 10;24(1):591. doi: 10.1186/s12877-024-05172-1.
Care transitions are high-risk processes, especially for people with complex or chronic illness. Discharge letters are an opportunity to provide written information to improve patients' self-management after discharge. The aim of this study is to determine the impact of discharge letter content on unplanned hospital readmissions and self-rated quality of care transitions among patients 60 years of age or older with chronic illness.
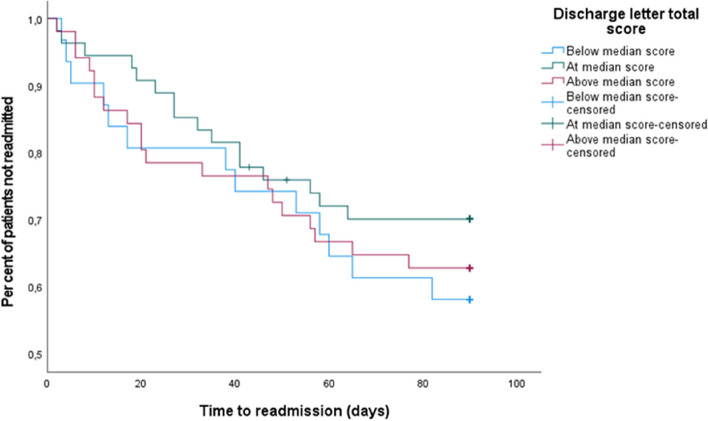
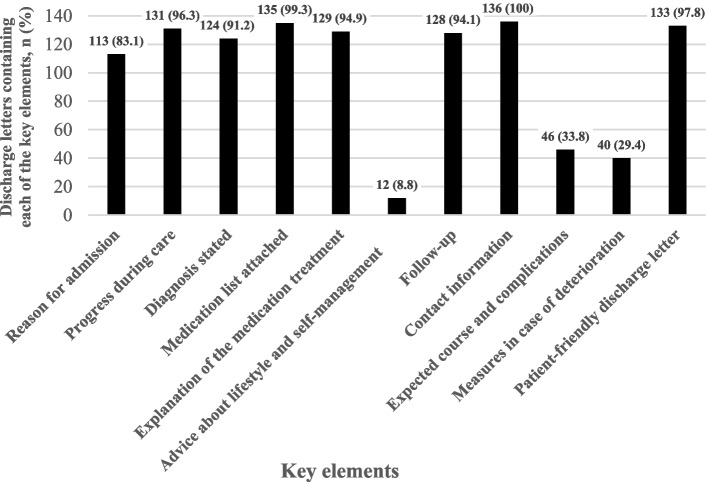
The study had a convergent mixed methods design. Patients with chronic obstructive pulmonary disease or congestive heart failure were recruited from two hospitals in Region Stockholm if they were living at home and Swedish-speaking. Patients with dementia or cognitive impairment, or a "do not resuscitate" statement in their medical record were excluded. Discharge letters from 136 patients recruited to a randomised controlled trial were coded using an assessment matrix and deductive content analysis. The assessment matrix was based on a literature review performed to identify key elements in discharge letters that facilitate a safe care transition to home. The coded key elements were transformed into a quantitative variable of "SAFE-D score". Bivariate correlations between SAFE-D score and quality of care transition as well as unplanned readmissions within 30 and 90 days were calculated. Lastly, a multivariable Cox proportional hazards model was used to investigate associations between SAFE-D score and time to readmission.
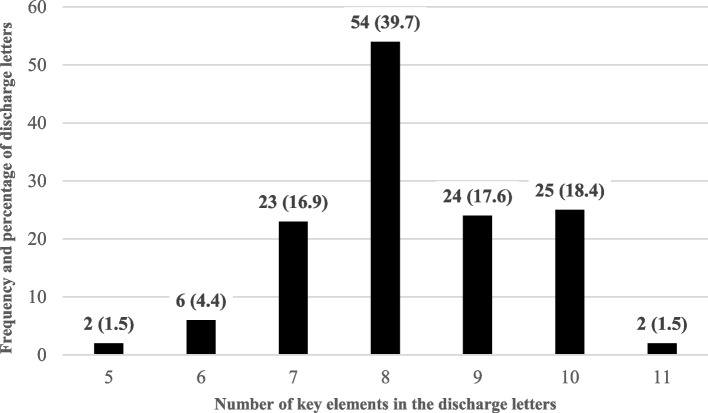
All discharge letters contained at least five of eleven key elements. In less than two per cent of the discharge letters, all eleven key elements were present. Neither SAFE-D score, nor single key elements correlated with 30-day or 90-day readmission rate. SAFE-D score was not associated with time to readmission when adjusted for a range of patient characteristics and self-rated quality of care transitions.
While written summaries play a role, they may not be sufficient on their own to ensure safe care transitions and effective self-care management post-discharge.
Clinical Trials. giv, NCT02823795, 01/09/2016.
交接过程风险较高,尤其是对患有复杂或慢性疾病的患者而言。出院小结是提供书面信息以改善患者出院后自我管理的机会。本研究旨在确定慢性疾病老年患者出院小结的内容对非计划性住院再入院和自我评估的交接质量的影响。
本研究采用收敛混合方法设计。如果患者居住在斯德哥尔摩地区的家中且能讲瑞典语,且患有慢性阻塞性肺疾病或充血性心力衰竭,则从两家医院招募他们参加这项研究。如果患者患有痴呆或认知障碍,或病历中有“不复苏”声明,则将其排除在外。从一项随机对照试验中招募的 136 名患者的出院小结使用评估矩阵和演绎内容分析法进行编码。评估矩阵是基于文献回顾确定的,以确定有助于安全居家交接的出院小结中的关键要素。编码的关键要素转化为“SAFE-D 评分”的定量变量。计算 SAFE-D 评分与交接质量以及 30 天和 90 天内非计划性再入院之间的相关性。最后,使用多变量 Cox 比例风险模型来研究 SAFE-D 评分与再入院时间之间的关联。
所有出院小结都至少包含十一个关键要素中的五个。不到两成的出院小结包含所有十一个关键要素。SAFE-D 评分或单个关键要素均与 30 天或 90 天再入院率无关。调整一系列患者特征和自我评估的交接质量后,SAFE-D 评分与再入院时间无关。
尽管书面摘要发挥了作用,但仅凭它们本身可能不足以确保安全交接和有效的出院后自我护理管理。
ClinicalTrials.gov,NCT02823795,2016 年 9 月 1 日。