Central Diagnostic Laboratory, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands.
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands.
J Med Internet Res. 2024 Jul 11;26:e54867. doi: 10.2196/54867.
Electronic informed consent (eIC) is increasingly used in clinical research due to several benefits including increased enrollment and improved efficiency. Within a learning health care system, a pilot was conducted with an eIC for linking data from electronic health records with national registries, general practitioners, and other hospitals.
We evaluated the eIC pilot by comparing the response to the eIC with the former traditional paper-based informed consent (IC). We assessed whether the use of eIC resulted in a different study population by comparing the clinical patient characteristics between the response categories of the eIC and former face-to-face IC procedure.
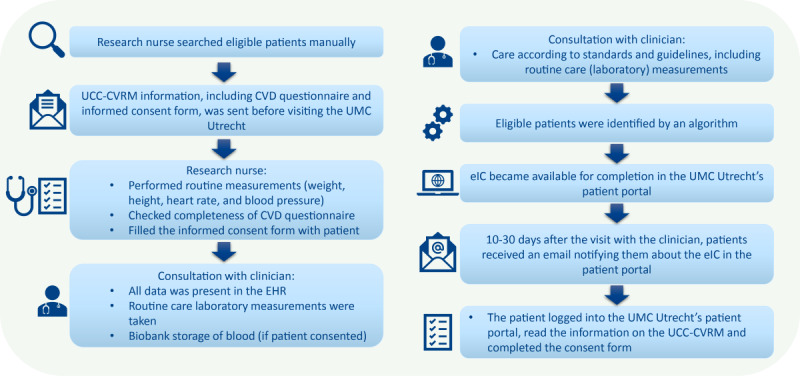
All patients with increased cardiovascular risk visiting the University Medical Center Utrecht, the Netherlands, were eligible for the learning health care system. From November 2021 to August 2022, an eIC was piloted at the cardiology outpatient clinic. Prior to the pilot, a traditional face-to-face paper-based IC approach was used. Responses (ie, consent, no consent, or nonresponse) were assessed and compared between the eIC and face-to-face IC cohorts. Clinical characteristics of consenting and nonresponding patients were compared between and within the eIC and the face-to-face cohorts using multivariable regression analyses.
A total of 2254 patients were included in the face-to-face IC cohort and 885 patients in the eIC cohort. Full consent was more often obtained in the eIC than in the face-to-face cohort (415/885, 46.9% vs 876/2254, 38.9%, respectively). Apart from lower mean hemoglobin in the full consent group of the eIC cohort (8.5 vs 8.8; P=.0021), the characteristics of the full consenting patients did not differ between the eIC and face-to-face IC cohorts. In the eIC cohort, only age differed between the full consent and the nonresponse group (median 60 vs 56; P=.0002, respectively), whereas in the face-to-face IC cohort, the full consent group seemed healthier (ie, higher hemoglobin, lower glycated hemoglobin [HbA], lower C-reactive protein levels) than the nonresponse group.
More patients provided full consent using an eIC. In addition, the study population remained broadly similar. The face-to-face IC approach seemed to result in a healthier study population (ie, full consenting patients) than the patients without IC, while in the eIC cohort, the characteristics between consent groups were comparable. Thus, an eIC may lead to a better representation of the target population, increasing the generalizability of results.
由于增加入组人数和提高效率等诸多益处,电子知情同意(eIC)在临床研究中得到了越来越多的应用。在学习型医疗保健系统中,对电子健康记录与国家登记处、全科医生和其他医院的数据进行链接的电子知情同意进行了试点。
通过比较电子知情同意与传统纸质知情同意的反应,评估电子知情同意的试点情况。我们通过比较电子知情同意和传统面对面知情同意程序的反应类别中的临床患者特征,评估了使用电子知情同意是否导致了不同的研究人群。
所有心血管风险增加的荷兰乌得勒支大学医学中心患者均符合学习型医疗保健系统的条件。从 2021 年 11 月到 2022 年 8 月,在心脏病学门诊进行了电子知情同意的试点。在试点之前,使用了传统的面对面纸质知情同意方法。评估了电子知情同意和面对面知情同意组的反应(即同意、不同意或无反应),并对其进行了比较。使用多变量回归分析比较了电子知情同意组和面对面知情同意组内和组间同意和不同意患者的临床特征。
共有 2254 名患者被纳入面对面知情同意组,885 名患者被纳入电子知情同意组。电子知情同意组的完全同意比例高于面对面知情同意组(415/885,46.9% vs 876/2254,38.9%)。除了电子知情同意组完全同意组的平均血红蛋白较低(8.5 与 8.8;P=.0021)外,电子知情同意组和面对面知情同意组的完全同意患者特征没有差异。在电子知情同意组中,只有年龄在完全同意组和无反应组之间存在差异(中位数分别为 60 与 56;P=.0002),而在面对面知情同意组中,完全同意组似乎比无反应组更健康(即血红蛋白较高,糖化血红蛋白[HbA]较低,C 反应蛋白水平较低)。
使用电子知情同意书的患者中有更多的人提供了完全同意。此外,研究人群基本保持相似。面对面知情同意方法似乎产生了一个更健康的研究人群(即完全同意的患者),而不是没有知情同意的患者,而在电子知情同意组中,同意组之间的特征是可比的。因此,电子知情同意可能会更好地代表目标人群,从而提高结果的可推广性。