Tatsumura Masaki, Kawamura Tokio, Uchida Ayako, Funayama Toru
Department of Orthopaedic Surgery and Sports Medicine, Tsukuba University Hospital Mito Clinical Education and Training Center/Mito Kyodo General Hospital, Mito, JPN.
Department of Orthopaedic Surgery, University of Tsukuba, Tsukuba, JPN.
Cureus. 2024 Jun 11;16(6):e62182. doi: 10.7759/cureus.62182. eCollection 2024 Jun.
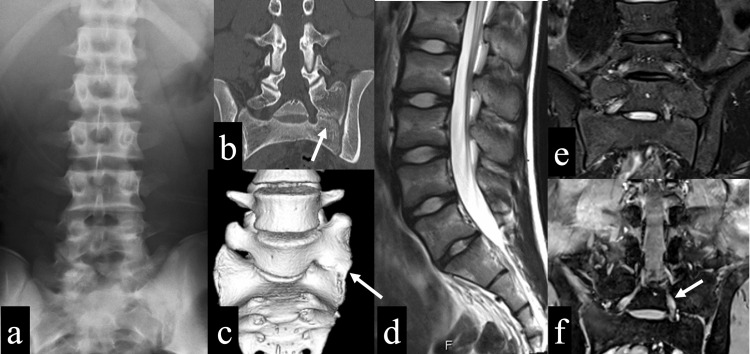
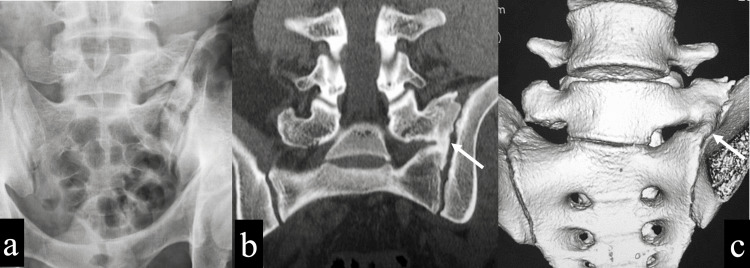
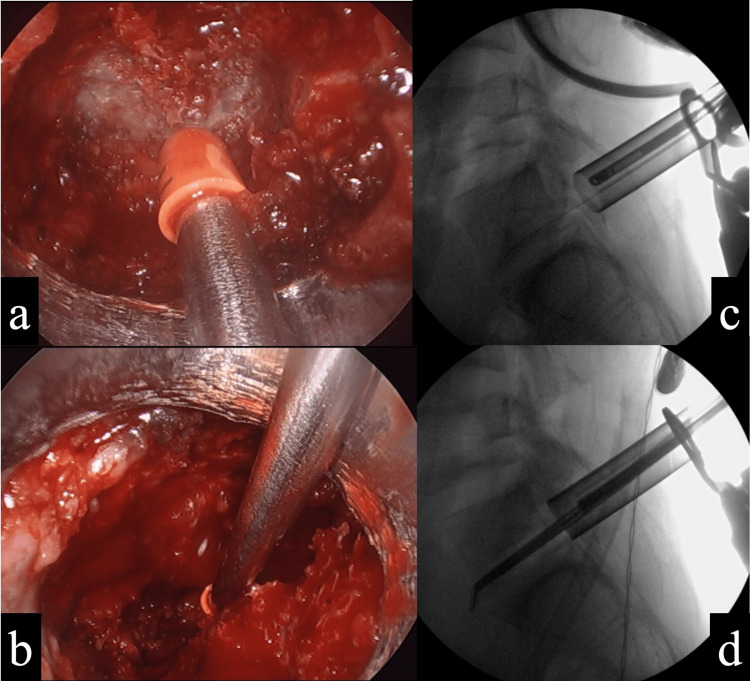
Bertolotti's syndrome is a syndrome in which the transverse process of the most caudal lumbar vertebra becomes enlarged and articulates with the sacral alar, causing back pain. Here, we report a case of an adolescent basketball player with Bertolotti's syndrome who was unable to resume playing despite conservative treatment and underwent an endoscopic partial transverse process and sacral alar resection. A 16-year-old male basketball player presented to our hospital with a chief complaint of left low back pain during exercise and prolonged sitting for over one month. No obvious neurological abnormality was found. X-rays and CT showed lumbosacral transitional vertebrae, and the left transverse process of the sixth lumbar vertebra articulated with the sacrum and iliac, which was the Castellvi classification IIA. A block injection into the articulated surface produced improvement in pain, but the effect was not sustained. Since the patient was refractory to conservative treatments, such as medication and physiotherapy, surgery was performed. During surgery, the articulated transverse process and sacral alar were partially resected endoscopically. Because of the proximity of the resection site to the S1 nerve root, intraoperative electromyography (free-run EMG) was used to detect nerve root irritation symptoms in real time. The patient had no postoperative complications, his low back pain improved immediately, and he returned to play basketball three months after surgery. One year after surgery, the bone resection site showed gradual bone regeneration, and two years after surgery, the transverse process and sacral alar showed a bony bridge. The transverse process was enlarged compared to immediately after surgery but remained smaller than that before surgery. The patient continued to play basketball for two years after surgery without back pain, and no symptoms due to bone regeneration appeared. In the present case, a partial resection of the transverse process and sacral alar was performed with good results. Because the bone resection site was close to the S1 nerve root, the use of an endoscope and intraoperative free-run EMG allowed for a safer procedure during the bone resection. In addition, the patient did not present with symptoms that would affect his basketball performance, although the bone regenerated and bridging occurred between the transverse process and sacral alar over a two-year postoperative course.
贝托洛蒂综合征是一种综合征,其中最尾侧腰椎的横突增大并与骶骨翼关节相连,导致背痛。在此,我们报告一例患有贝托洛蒂综合征的青少年篮球运动员,尽管经过保守治疗仍无法恢复比赛,遂接受了内镜下部分横突和骶骨翼切除术。一名16岁男性篮球运动员因运动及长时间久坐后左侧下腰痛为主诉就诊于我院,病程超过1个月。未发现明显神经异常。X线和CT显示腰骶部移行椎,第六腰椎左侧横突与骶骨和髂骨相连,属于卡斯特尔维分类IIA。关节面阻滞注射使疼痛有所改善,但效果未持续。由于患者对药物和物理治疗等保守治疗无效,故行手术治疗。手术中,在内镜下部分切除关节横突和骶骨翼。由于切除部位靠近S1神经根,术中使用肌电图(自由运行肌电图)实时检测神经根刺激症状。患者术后无并发症,下腰痛立即改善,术后3个月恢复打篮球。术后1年,骨切除部位显示逐渐骨再生,术后2年,横突和骶骨翼显示骨桥形成。与术后即刻相比,横突增大,但仍小于术前。患者术后继续打篮球2年无背痛,未出现骨再生相关症状。在本病例中,部分切除横突和骶骨翼取得了良好效果。由于骨切除部位靠近S1神经根,使用内镜和术中自由运行肌电图使骨切除过程更安全。此外,尽管术后两年内横突和骶骨翼之间发生了骨再生和骨桥形成,但患者未出现影响其篮球表现的症状。