Veskimae Erik, Subbarayan Selvarani, Campi Riccardo, Carron Domitille, Omar Muhammad Imran, Yuan Cathy, Dimitropoulos Konstantinos, Van Hemelrijck Mieke, Bryan Richard T, N'Dow James, Babjuk Marek, Alfred Witjes J, Sylvester Richard, MacLennan Steven
Department of Urology, Tampere University Hospital, Tampere, Finland.
Academic Urology Unit, University of Aberdeen, Aberdeen, UK.
Bladder Cancer. 2021 May 25;7(2):221-241. doi: 10.3233/BLC-201510. eCollection 2021.
Heterogenous outcome reporting in non-muscle-invasive bladder cancer (NMIBC) effectiveness trials of adjuvant treatment after transurethral resection (TURBT) has been noted in systematic reviews (SRs). This hinders comparing results across trials, combining them in meta-analyses, and evidence-based decision-making for patients and clinicians.
We aimed to systematically review the extent of reporting and definition heterogeneity.
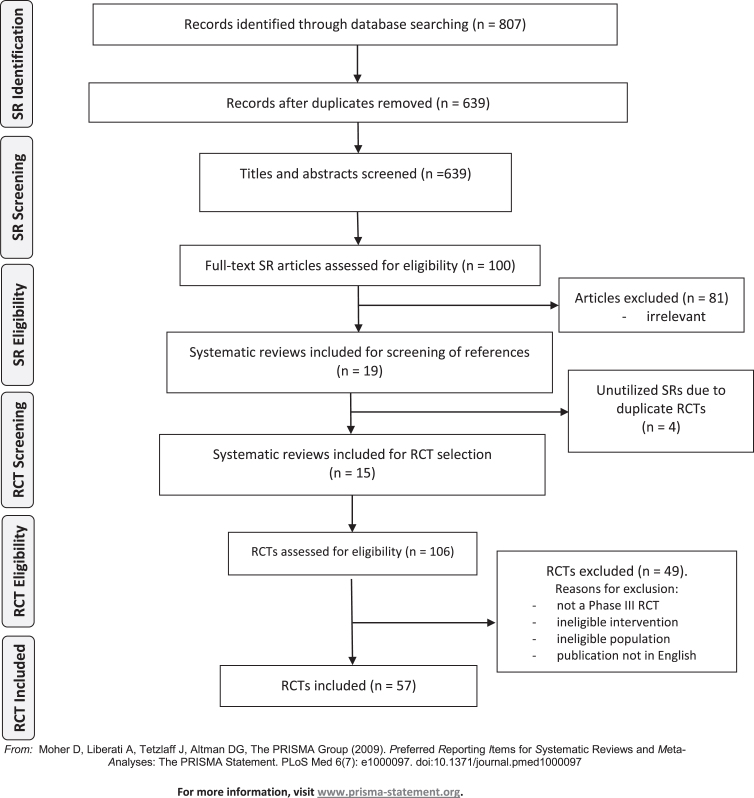
We included randomized controlled trials (RCTs) identified from SRs comparing adjuvant treatments after TURBT or TURBT alone in patients with NMIBC (with or without carcinoma ) published between 2000-2020. Abstracts and full texts were screened independently by two reviewers. Data were extracted by one reviewer and checked by another.
We screened 807 abstracts; from 15 SRs, 57 RCTs were included. Verbatim outcome names were coded to standard outcome names and organised using the Williamson and Clarke taxonomy. Recurrence (98%), progression (74%), treatment response (in CIS studies) (40%), and adverse events (77%) were frequently reported across studies. However, overall (33%) and cancer-specific (33%) survival, treatment completion (17%) and treatment change (37%) were less often reported. Quality of Life (3%) and economic outcomes (2%) were rarely reported. Heterogeneity was evident throughout, particularly in the definitions of progression and recurrence, and how CIS patients were handled in the analysis of studies with predominantly papillary patients, highlighting further issues with the definition of recurrence and progression vs treatment response for CIS patients. Data reporting was also inconsistent, with some trials reporting event rates at various time-points and others reporting time-to-event with or without Hazard Ratios. Adverse events were inconsistently reported. QoL data was absent in most trials.
Heterogenous outcome reporting is evident in NMIBC effectiveness trials. This has profound implications for meta-analyses, SRs and evidence-based treatment decisions. A core outcome set is required to reduce heterogeneity.
This systematic review found inconsistencies in outcome definitions and reporting, pointing out the urgent need for a core outcome set to help improve evidence-based treatment decisions.
在系统评价(SR)中已注意到经尿道膀胱肿瘤切除术(TURBT)后辅助治疗的非肌层浸润性膀胱癌(NMIBC)有效性试验中存在异质性结果报告。这阻碍了跨试验比较结果、在荟萃分析中合并结果以及为患者和临床医生提供基于证据的决策。
我们旨在系统评价报告范围和定义异质性的程度。
我们纳入了从SR中识别出的随机对照试验(RCT),这些试验比较了2000年至2020年间NMIBC(有或无癌)患者TURBT后辅助治疗或单纯TURBT。摘要和全文由两名审阅者独立筛选。数据由一名审阅者提取并由另一名审阅者检查。
我们筛选了807篇摘要;从15项SR中,纳入了57项RCT。逐字记录的结果名称被编码为标准结果名称,并使用威廉姆森和克拉克分类法进行整理。复发(98%)、进展(74%)、治疗反应(在原位癌研究中)(40%)和不良事件(7%)在各项研究中经常被报告。然而,总生存率(33%)和癌症特异性生存率(33%)、治疗完成率(17%)和治疗改变率(37%)报告较少。生活质量(3%)和经济结果(2%)很少被报告。异质性在整个过程中都很明显,特别是在进展和复发的定义以及在以乳头状患者为主的研究分析中如何处理原位癌患者方面,这突出了原位癌患者复发和进展与治疗反应定义的进一步问题。数据报告也不一致,一些试验报告了不同时间点的事件发生率,而另一些试验报告了事件发生时间,有或没有风险比。不良事件报告不一致。大多数试验中缺乏生活质量数据。
NMIBC有效性试验中存在明显的异质性结果报告。这对荟萃分析、SR和基于证据的治疗决策有深远影响。需要一个核心结局集来减少异质性。
这项系统评价发现结果定义和报告存在不一致,指出迫切需要一个核心结局集来帮助改善基于证据的治疗决策。