Angelis Mario de, Siech Carolin, Di Bello Francesco, Peñaranda Natali Rodriguez, Goyal Jordan A, Tian Zhe, Longo Nicola, Chun Felix K H, Puliatti Stefano, Saad Fred, Shariat Shahrokh F, Longoni Mattia, Gandaglia Giorgio, Moschini Marco, Montorsi Francesco, Briganti Alberto, Karakiewicz Pierre I
Cancer Prognostics and Health Outcomes Unit, Division of Urology, University of Montréal Health Center, Montréal, QC H2X 3E4, Canada.
Division of Experimental Oncology, Unit of Urology, URI, IRCCS Ospedale San Raffaele, 20132 Milan, Italy.
Cancers (Basel). 2024 Jun 29;16(13):2404. doi: 10.3390/cancers16132404.
Historical external beam radiation therapy (EBRT) for rectosigmoid cancer (RCa) predisposed patients to an increased risk of secondary bladder cancer (BCa). However, no contemporary radiotherapy studies are available. We addressed this knowledge gap.
Within the Surveillance, Epidemiology, and End Results database (2000-2020), we identified non-metastatic RCa patients who either underwent radiotherapy (EBRT+) or did not (EBRT-). Cumulative incidence plots and multivariable competing risk regression models (CRR) were fitted to address rates of BCa after RCa. In the subgroup of BCa patients, the same methodology addressed BCa-specific mortality (BCSM) according to EBRT exposure status.
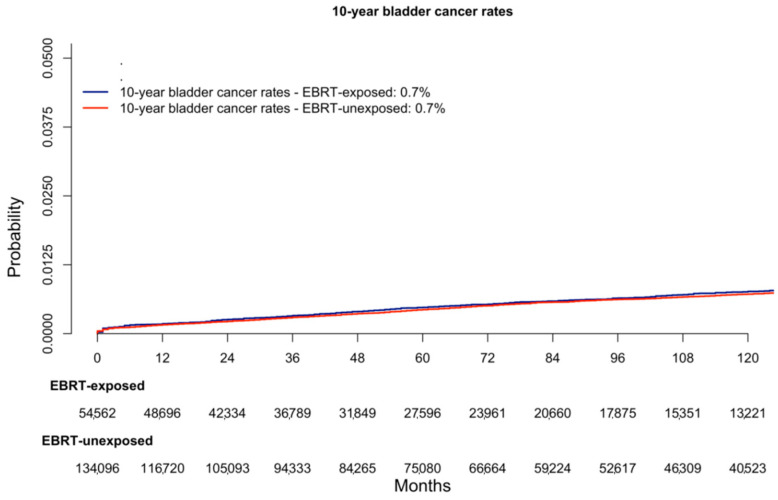
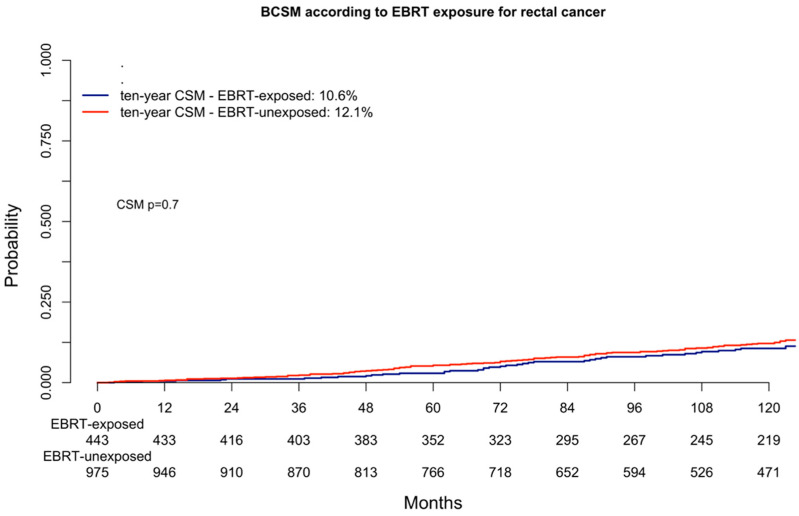
Of the 188,658 non-metastatic RCa patients, 54,562 (29%) were EBRT+ vs. 134,096 (73%) who were EBRT-. In the cumulative incidence plots, the ten-year BCa rates were 0.7% in EBRT+ vs. 0.7% in EBRT- patients ( = 0.8). In the CRR, EBRT+ status was unrelated to BCa rates (multivariable HR: 1.1, = 0.8). In the subgroup of 1416 patients with BCa after RCa, 443 (31%) were EBRT+ vs. 973 (69%) who were EBRT-. In the cumulative incidence plots, the ten-year BCSM rates were 10.6% in EBRT+ vs. 12.1% in EBRT- patients ( = 0.7). In the CRR, EBRT+ status was unrelated to subsequent BCSM rates (multivariable HR: 0.9, = 0.9).
Although historical EBRT for RCa predisposed patients to higher BCa rates, contemporary EBRT for RCa is not associated with increased subsequent BCa risk. Moreover, in patients with BCa after RCa, exposure to EBRT does not affect BCSM.
既往用于治疗直肠乙状结肠癌(RCa)的外照射放疗(EBRT)使患者患继发性膀胱癌(BCa)的风险增加。然而,目前尚无当代放疗研究。我们填补了这一知识空白。
在监测、流行病学和最终结果数据库(2000 - 2020年)中,我们确定了接受放疗(EBRT+)或未接受放疗(EBRT-)的非转移性RCa患者。采用累积发病率图和多变量竞争风险回归模型(CRR)来分析RCa后BCa的发生率。在BCa患者亚组中,采用相同方法根据EBRT暴露状态分析BCa特异性死亡率(BCSM)。
在188,658例非转移性RCa患者中,54,562例(29%)接受了EBRT,134,096例(73%)未接受EBRT。在累积发病率图中,EBRT+患者的十年BCa发生率为0.7%,EBRT-患者为0.7%(P = 0.8)。在CRR中,EBRT+状态与BCa发生率无关(多变量风险比:1.1,P = 0.8)。在1416例RCa后发生BCa的患者亚组中,443例(31%)接受了EBRT,973例(69%)未接受EBRT。在累积发病率图中,EBRT+患者的十年BCSM发生率为10.6%,EBRT-患者为12.1%(P = 0.7)。在CRR中,EBRT+状态与随后的BCSM发生率无关(多变量风险比:0.9,P = 0.9)。
尽管既往用于RCa的EBRT使患者患BCa的风险更高,但当代用于RCa的EBRT与随后BCa风险增加无关。此外,在RCa后发生BCa的患者中接受EBRT并不影响BCSM。