Pereira Chantal F R, Dijxhoorn Anne-Floor Q, Koekoek Berdine, van den Broek Monique, van der Steen Karin, Engel Marijanne, van Rijn Marjon, Meijers Judith M, Hasselaar Jeroen, van der Heide Agnes, Onwuteaka-Philipsen Bregje D, van den Beuken-van Everdingen Marieke H J, van der Linden Yvette M, Boddaert Manon S, Jeurissen Patrick P T, Merkx Matthias A W, Raijmakers Natasja J H
Netherlands Comprehensive Cancer Organisation (IKNL), Utrecht, The Netherlands.
Netherlands Association for Palliative Care, Utrecht, The Netherlands.
Int J Integr Care. 2024 Jul 8;24(3):6. doi: 10.5334/ijic.7504. eCollection 2024 Jul-Sep.
This study aimed to assess the effect of integrated palliative care (IPC) on potentially inappropriate end- of-life care and healthcare-costs in the last 30 days of life in the Netherlands.
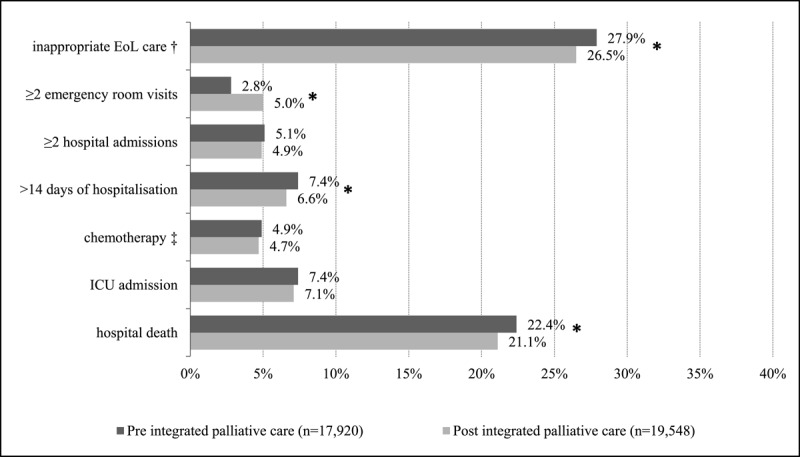
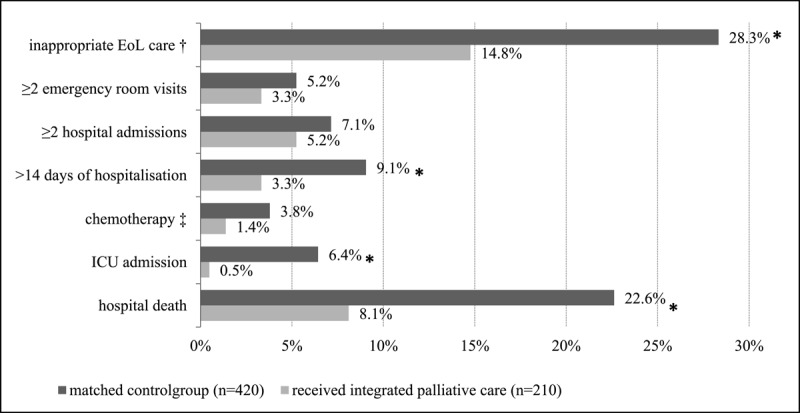
Nationwide health-insurance claims data were used to assess potentially inappropriate end-of-life care (≥2 emergency room visits; ≥2 hospital admissions; >14 days hospitalization; chemotherapy; ICU admission; hospital death) and healthcare-costs in all deceased adults in IPC regions pre- and post- implementation and in those receiving IPC compared to a 1:2 matched control group.
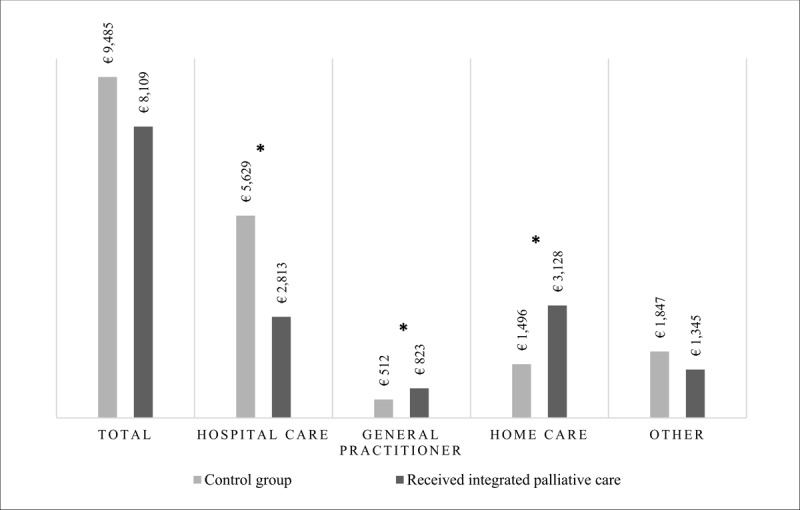
In regions providing IPC deceased adults (n = 37,468) received significantly less potentially inappropriate end-of-life care post-implementation compared to pre-implementation (26.5% vs 27.9%; p < 0.05). Deceased adults who received IPC (n = 210) also received significantly less potentially inappropriate end-of-life care compared to a matched control group (14.8% vs 28.3%; p < 0.05). Mean hospital costs significantly decreased for deceased adults who received IPC (€2,817), while mean costs increased for general practitioner services (€311) and home care (€1,632).
These results highlight the importance of implementation of integrated palliative care and suitable payment. Further research in a larger sample is needed.
This study shows less potentially inappropriate end-of-life care and a shift in healthcare costs from hospital to general practitioner and home care with IPC.
本研究旨在评估荷兰综合姑息治疗(IPC)对生命最后30天潜在不适当的临终护理及医疗费用的影响。
使用全国医疗保险理赔数据,评估IPC实施前后IPC地区所有成年死者以及接受IPC者与1:2匹配对照组相比的潜在不适当的临终护理(≥2次急诊就诊;≥2次住院;住院超过14天;化疗;入住重症监护病房;在医院死亡)及医疗费用。
在提供IPC的地区,成年死者(n = 37,468)实施后接受潜在不适当临终护理的比例显著低于实施前(26.5%对27.9%;p < 0.05)。接受IPC的成年死者(n = 210)与匹配对照组相比,接受潜在不适当临终护理的比例也显著更低(14.8%对28.3%;p < 0.05)。接受IPC的成年死者的平均住院费用显著降低(2817欧元),而全科医生服务(311欧元)和家庭护理(1632欧元)的平均费用增加。
这些结果凸显了实施综合姑息治疗及适当付费的重要性。需要在更大样本中进行进一步研究。
本研究表明,IPC可减少潜在不适当的临终护理,并使医疗费用从医院转向全科医生服务和家庭护理。