Asano Yuta, Veatch Joshua, McAfee Megan, Bakhtiari Jakob, Lee Bo, Martin Lauren, Zhang Shihong, Mazziotta Francesco, Paulson Kelly G, Schmitt Thomas M, Munkbhat Ariunnaa, Young Cecilia, Seaton Brandon, Hunter Daniel, Horst Nick, Lindberg Marcus, Miller Natalie, Stone Matt, Bielas Jason, Koelle David, Voillet Valentin, Gottardo Raphael, Gooley Ted, Oda Shannon, Greenberg Philip D, Nghiem Paul, Chapuis Aude G
Fred Hutchinson Cancer Center, Seattle, WA, USA.
University of Washington, Seattle, WA, USA.
medRxiv. 2024 Jul 5:2024.07.01.24309780. doi: 10.1101/2024.07.01.24309780.
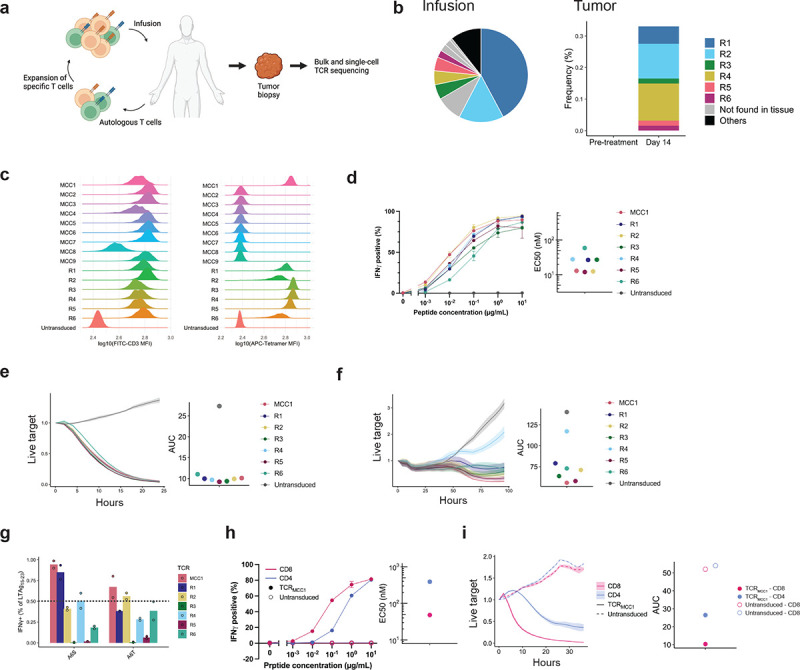
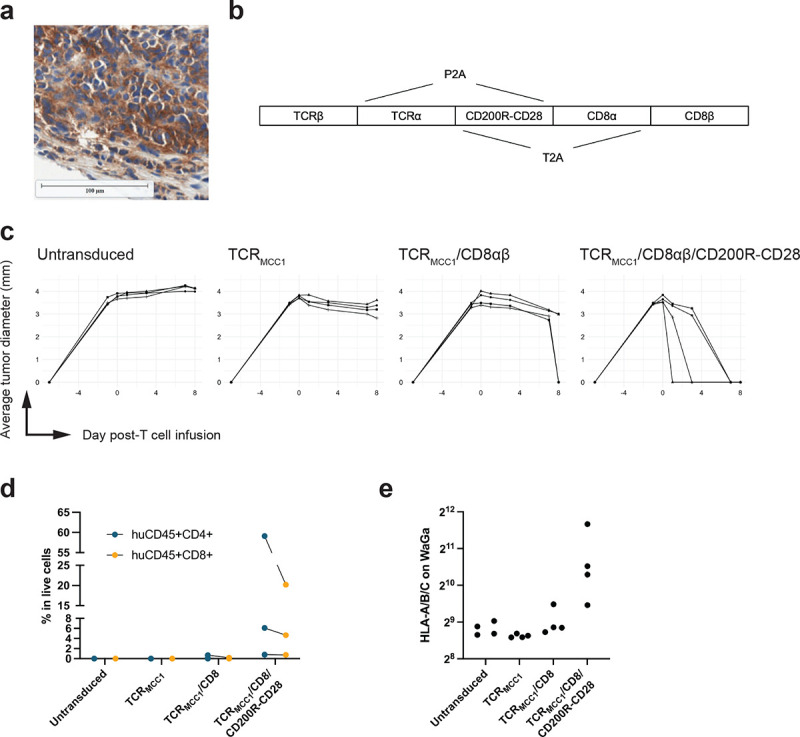
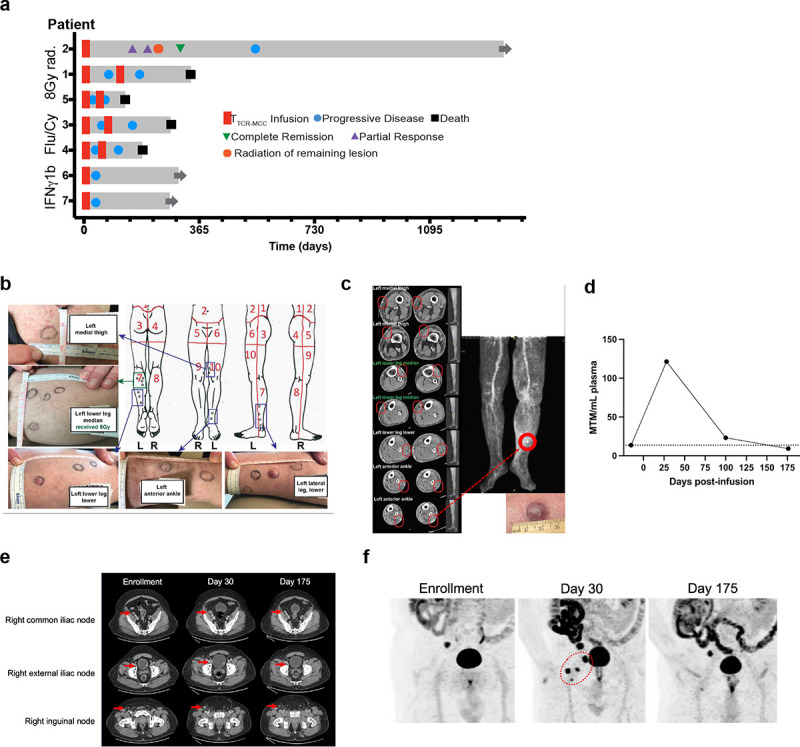
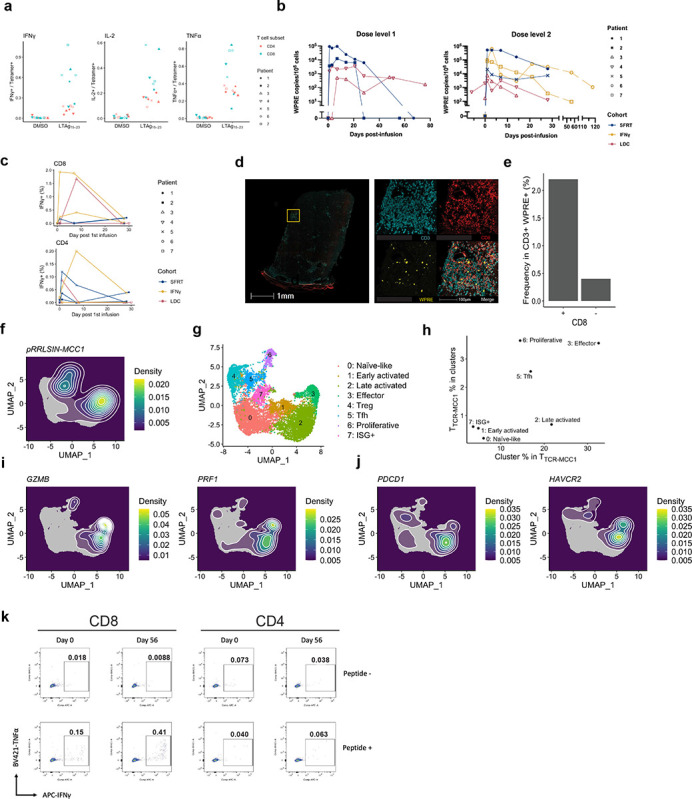
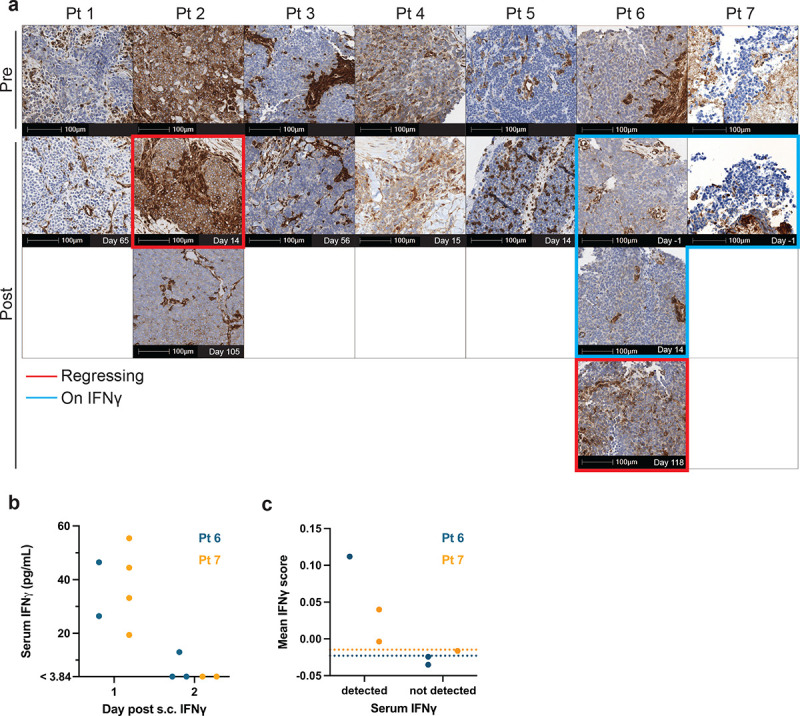
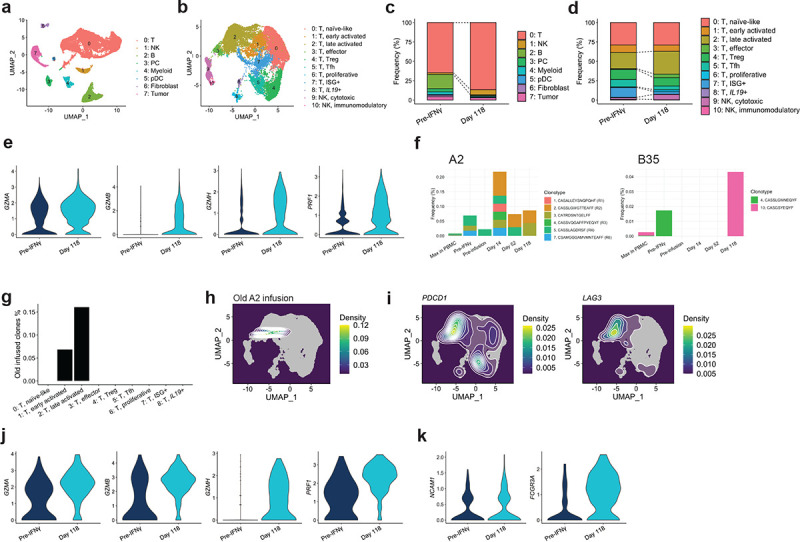
Although immune check-point inhibitors (CPIs) revolutionized treatment of Merkel cell carcinoma (MCC), patients with CPI-refractory MCC lack effective therapy. More than 80% of MCC express T-antigens encoded by Merkel cell polyomavirus, which is an ideal target for T-cell receptor (TCR)-based immunotherapy. However, MCC often repress HLA expression, requiring additional strategies to reverse the downregulation for allowing T cells to recognize their targets. We identified TCR that recognizes a T-antigen epitope restricted to human leukocyte antigen (HLA)-A*02:01. Seven CPI-refractory metastatic MCC patients received CD4 and CD8 T cells transduced with TCR (T) preceded either by lymphodepleting chemotherapy or an HLA-upregulating regimen (single-fraction radiation therapy (SFRT) or systemic interferon gamma (IFNγ)) with concurrent avelumab. Two patients who received preceding SFRT and IFNγ respectively experienced tumor regression. One experienced regression of 13/14 subcutaneous lesions with 1 'escape' lesion and the other had delayed tumor regression in all lesions after initial progression. Although T cells with an activated phenotype infiltrated tumors including the 'escape' lesion, all progressing lesions transcriptionally lacked HLA expression. While SFRT/IFNγ did not immediately upregulate tumor HLA expression, a secondary endogenous antigen-specific T cell infiltrate was detected in one of the regressing tumors and associated with HLA upregulation, indicating in situ immune responses have the potential to reverse HLA downregulation. Indeed, supplying a strong co-stimulatory signal via a CD200R-CD28 switch receptor allows T cells to control HLA-downregulated MCC cells in a xenograft mouse model, upregulating HLA expression. Our results demonstrate the potential of TCR gene therapy for metastatic MCC and propose a next strategy for overcoming epigenetic downregulation of HLA in MCC.
尽管免疫检查点抑制剂(CPI)彻底改变了默克尔细胞癌(MCC)的治疗方式,但对CPI难治的MCC患者仍缺乏有效的治疗方法。超过80%的MCC表达由默克尔细胞多瘤病毒编码的T抗原,这是基于T细胞受体(TCR)的免疫治疗的理想靶点。然而,MCC常常抑制HLA表达,需要额外的策略来逆转这种下调,以使T细胞能够识别其靶点。我们鉴定出了一种识别限于人类白细胞抗原(HLA)-A*02:01的T抗原表位的TCR。7例对CPI难治的转移性MCC患者接受了转导有TCR的CD4和CD8 T细胞,在输注前先进行淋巴细胞清除化疗或采用HLA上调方案(单次分割放射治疗(SFRT)或全身干扰素γ(IFNγ))并同时使用阿维鲁单抗。分别接受SFRT和IFNγ预处理的2例患者出现了肿瘤消退。1例患者14个皮下病灶中有13个消退,有1个“逃逸”病灶,另1例患者在初始进展后所有病灶均出现延迟肿瘤消退。尽管具有活化表型的T细胞浸润了包括“逃逸”病灶在内的肿瘤,但所有进展性病灶在转录水平上均缺乏HLA表达。虽然SFRT/IFNγ并未立即上调肿瘤HLA表达,但在一个消退的肿瘤中检测到了继发性内源性抗原特异性T细胞浸润,并与HLA上调相关,表明原位免疫反应有可能逆转HLA下调。事实上,通过CD200R-CD28开关受体提供强共刺激信号可使T细胞在异种移植小鼠模型中控制HLA下调的MCC细胞,上调HLA表达。我们的结果证明了TCR基因治疗转移性MCC的潜力,并提出了克服MCC中HLA表观遗传下调的下一步策略。