Division of Emergency Medicine, Ann & Robert Lurie Children's Hospital, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Department of Pediatrics, Dell Medical School at the University of Texas at Austin.
JAMA Netw Open. 2024 Jul 1;7(7):e2422196. doi: 10.1001/jamanetworkopen.2024.22196.
Classifying hospitals across a wide range of pediatric capabilities, including medical, surgical, and specialty services, would improve understanding of access and outcomes.
To develop a classification system for hospitals' pediatric capabilities.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included data from 2019 on all acute care hospitals with emergency departments in 10 US states that treated at least 1 child per day. Statistical analysis was performed from September 2023 to February 2024.
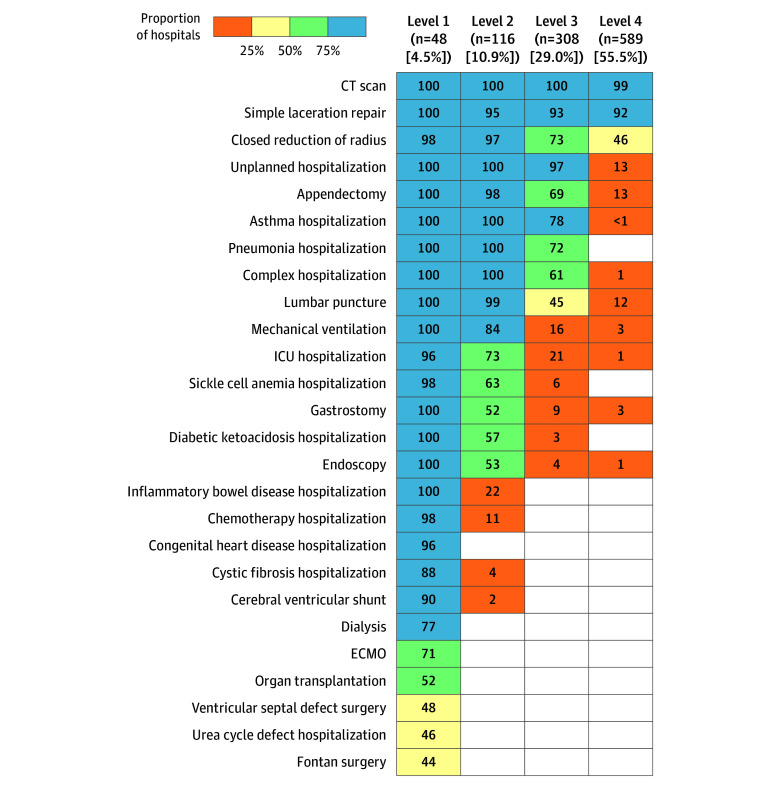
Pediatric hospital capability level, defined using latent class analysis. The latent class model parameters were the presence or absence of 26 functional capabilities, which ranged from performing laceration repairs to performing organ transplants. A simplified approach to categorization was derived and externally validated by comparing each hospital's latent class model classification with its simplified classification using data from 3 additional states.
Health care utilization and structural characteristics, including inpatient beds, pediatric intensive care unit (PICU) beds, and referral rates (proportion of patients transferred among patients unable to be discharged).
Using data from 1061 hospitals (716 metropolitan [67.5%]) with a median of 2934 pediatric ED encounters per year (IQR, 1367-5996), the latent class model revealed 4 pediatric levels, with a median confidence of hospital assignment to level of 100% (IQR, 99%-100%). Of 26 functional capabilities, level 1 hospitals had a median of 24 capabilities (IQR, 21-25), level 2 hospitals had a median of 13 (IQR, 11-15), level 3 hospitals had a median of 8 (IQR, 6-9), and level 4 hospitals had a median of 3 (IQR, 2-3). Pediatric level 1 hospitals had a median of 66 inpatient beds (IQR, 42-86), level 2 hospitals had a median of 16 (IQR, 9-22), level 3 hospitals had a median of 0 (IQR, 0-6), and level 4 hospitals had a median of 0 (IQR, 0-0) (P < .001). Level 1 hospitals had a median of 19 PICU beds (IQR, 10-28), level 2 hospitals had a median of 0 (IQR, 0-5), level 3 hospitals had a median of 0 (IQR, 0-0), and level 4 hospitals had a median of 0 (IQR, 0-0) (P < .001). Level 1 hospitals had a median referral rate of 1% (IQR, 1%-3%), level 2 hospitals had a median of 25% (IQR, 9%-45%), level 3 hospitals had a median of 70% (IQR, 52%-84%), and level 4 hospitals had a median of 100% (IQR, 98%-100%) (P < .001).
In this cross-sectional study of hospitals from 10 US states, a system to classify hospitals' pediatric capabilities in 4 levels was developed and was associated with structural and health care utilization characteristics. This system can be used to understand and track national pediatric acute care access and outcomes.
对广泛儿科能力的医院进行分类,包括医疗、外科和专科服务,将有助于更好地了解获得医疗服务的途径和结果。
开发一种用于医院儿科能力的分类系统。
设计、地点和参与者:本横断面研究纳入了来自美国 10 个州的 2019 年所有具有急诊部门且每天至少治疗 1 名儿童的急性护理医院的数据。统计分析于 2023 年 9 月至 2024 年 2 月进行。
儿科医院能力水平,使用潜在类别分析定义。潜在类别模型的参数是存在或不存在 26 种功能能力,范围从进行裂伤修复到进行器官移植。采用简化方法进行分类,并通过使用来自 3 个额外州的数据对每个医院的潜在类别模型分类与其简化分类进行外部验证。
医疗保健利用和结构特征,包括住院床位、儿科重症监护病房(PICU)床位和转诊率(无法出院的患者中被转诊的患者比例)。
在来自 1061 家(67.5%为大都市)医院的数据中(中位数为每年 2934 次儿科急诊就诊,IQR,1367-5996),潜在类别模型揭示了 4 个儿科水平,医院分配到水平的中位数置信度为 100%(IQR,99%-100%)。在 26 种功能能力中,1 级医院的中位数为 24 种能力(IQR,21-25),2 级医院的中位数为 13 种(IQR,11-15),3 级医院的中位数为 8 种(IQR,6-9),4 级医院的中位数为 3 种(IQR,2-3)。儿科 1 级医院的中位数为 66 张住院床位(IQR,42-86),2 级医院的中位数为 16 张(IQR,9-22),3 级医院的中位数为 0(IQR,0-6),4 级医院的中位数为 0(IQR,0-0)(P<0.001)。1 级医院的中位数为 19 张 PICU 床位(IQR,10-28),2 级医院的中位数为 0(IQR,0-5),3 级医院的中位数为 0(IQR,0-0),4 级医院的中位数为 0(IQR,0-0)(P<0.001)。1 级医院的中位数转诊率为 1%(IQR,1%-3%),2 级医院的中位数为 25%(IQR,9%-45%),3 级医院的中位数为 70%(IQR,52%-84%),4 级医院的中位数为 100%(IQR,98%-100%)(P<0.001)。
在这项对美国 10 个州医院的横断面研究中,开发了一种将医院儿科能力分为 4 个等级的系统,并与结构和医疗保健利用特征相关联。该系统可用于了解和跟踪全国儿科急性护理的获得途径和结果。