Population Health and Optimal Health Practices Research Unit, Trauma-Emergency-Critical Care Medicine, Centre de Recherche du CHU de Québec-Université Laval (Hôpital de l'Enfant-Jésus), Québec City, Québec, Canada.
Department of Social and Preventative Medicine, Université Laval, Québec, Québec, Canada.
JAMA Netw Open. 2023 Sep 5;6(9):e2334266. doi: 10.1001/jamanetworkopen.2023.34266.
Adult trauma centers (ATCs) have been shown to decrease injury mortality and morbidity in major trauma, but a synthesis of evidence for pediatric trauma centers (PTCs) is lacking.
To assess the effectiveness of PTCs compared with ATCs, combined trauma centers (CTCs), or nondesignated hospitals in reducing mortality and morbidity among children admitted to hospitals following trauma.
MEDLINE, Embase, and Web of Science through March 2023.
Studies comparing PTCs with ATCs, CTCs, or nondesignated hospitals for pediatric trauma populations (aged ≤19 years).
This systematic review and meta-analysis was performed following the Preferred Reporting Items for Systematic Review and Meta-analysis and Meta-analysis of Observational Studies in Epidemiology guidelines. Pairs of reviewers independently extracted data and evaluated risk of bias using the Risk of Bias in Nonrandomized Studies of Interventions tool. A meta-analysis was conducted if more than 2 studies evaluated the same intervention-comparator-outcome and controlled minimally for age and injury severity. Subgroup analyses were planned for age, injury type and severity, trauma center designation level and verification body, country, and year of conduct. Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess certainty of evidence.
MAIN OUTCOME(S) AND MEASURE(S): Primary outcomes were mortality, complications, functional status, discharge destination, and quality of life. Secondary outcomes were resource use and processes of care, including computed tomography (CT) and operative management of blunt solid organ injury (SOI).
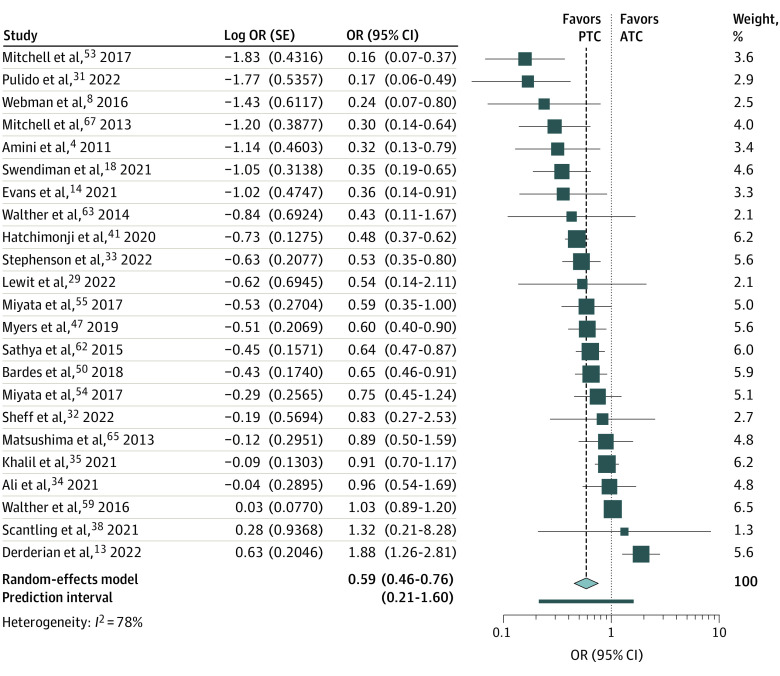
A total of 56 studies with 286 051 participants were included overall, and 34 were included in the meta-analysis. When compared with ATCs, PTCs were associated with a 41% lower risk of mortality (OR, 0.59; 95% CI, 0.46-0.76), a 52% lower risk of CT use (OR, 0.48; 95% CI, 0.26-0.89) and a 64% lower risk of operative management for blunt SOI (OR, 0.36; 95% CI, 0.23-0.57). The OR for complications was 0.80 (95% CI, 0.41-1.56). There was no association for mortality for older children (OR, 0.71; 95% CI, 0.47-1.06), and the association was closer to the null when PTCs were compared with CTCs (OR, 0.73; 95% CI, 0.53-0.99). Results remained similar for other subgroup analyses. GRADE certainty of evidence was very low for all outcomes.
In this systematic review and meta-analysis, results suggested that PTCs were associated with lower odds of mortality, CT use, and operative management for SOI than ATCs for children admitted to hospitals following trauma, but certainty of evidence was very low. Future studies should strive to address selection and confounding biases.
成人创伤中心(ATC)已被证明可降低严重创伤患者的死亡率和发病率,但缺乏儿科创伤中心(PTC)的证据综合。
评估 PTC 与 ATC、综合创伤中心(CTC)或非指定医院相比,在降低因创伤住院的儿童死亡率和发病率方面的效果。
通过 MEDLINE、Embase 和 Web of Science 检索 2023 年 3 月之前的文献。
比较 PTC 与 ATC、CTC 或非指定医院用于儿科创伤人群(年龄≤19 岁)的研究。
本系统评价和荟萃分析遵循系统评价和荟萃分析报告的首选项目和流行病学观察性研究荟萃分析的指南进行。如果超过 2 项研究评估了相同的干预措施-比较-结局,并对年龄和损伤严重程度进行了最小控制,则由两名评审员独立提取数据并使用干预措施风险评估工具评估偏倚风险。如果计划进行亚组分析,则包括年龄、损伤类型和严重程度、创伤中心指定级别和验证机构、国家和开展年份。使用推荐评估、制定和评估(GRADE)对证据的确定性进行评级。
主要结局是死亡率、并发症、功能状态、出院去向和生活质量。次要结局是资源利用和护理过程,包括计算机断层扫描(CT)和钝性实体器官损伤(SOI)的手术管理。
共有 56 项研究,涉及 286051 名参与者,其中 34 项研究纳入荟萃分析。与 ATC 相比,PTC 与死亡率降低 41%相关(OR,0.59;95%CI,0.46-0.76)、CT 使用率降低 52%相关(OR,0.48;95%CI,0.26-0.89)和钝性 SOI 的手术管理降低 64%相关(OR,0.36;95%CI,0.23-0.57)。并发症的 OR 为 0.80(95%CI,0.41-1.56)。对于年龄较大的儿童,死亡率没有相关性(OR,0.71;95%CI,0.47-1.06),当与 CTC 比较时,相关性更接近无效(OR,0.73;95%CI,0.53-0.99)。其他亚组分析结果相似。所有结局的证据确定性均为极低。
在本系统评价和荟萃分析中,结果表明,与 ATC 相比,PTC 与儿童创伤后住院死亡率、CT 使用率和 SOI 手术管理的可能性降低相关,但证据确定性极低。未来的研究应努力解决选择和混杂偏倚。