Department of Pulmonology and Respiratory Medicine, Lung Center Stuttgart - Schillerhoehe Lung Clinic GmbH, affiliated with Robert-Bosch-Hospital GmbH (Bosch Health Campus), Auerbachstr. 110, Stuttgart, 70376, Germany.
Comprehensive Pneumology Center (CPC-M), Member of the German Center for Lung Research (DZL), Munich, Germany.
BMC Pulm Med. 2024 Jul 16;24(1):345. doi: 10.1186/s12890-024-03151-1.
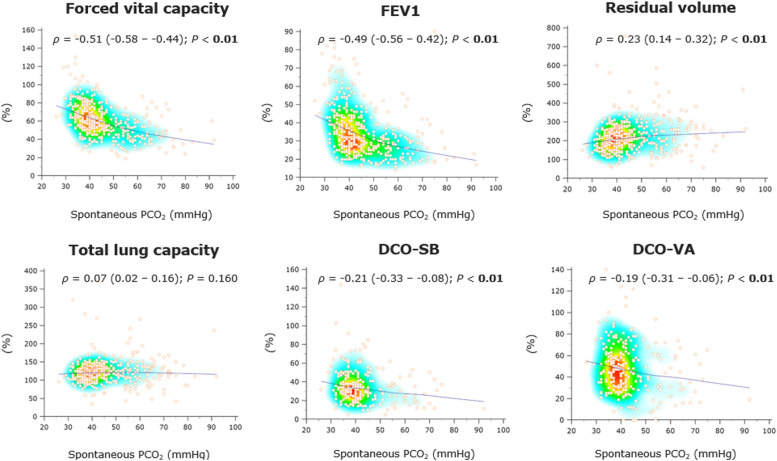
In advanced chronic obstructive pulmonary disease (COPD), hypercapnia may occur due to severe bronchial obstruction with lung hyperinflation. Non-invasive ventilation (NIV) provides the standard of care intended to achieve physiological PCO levels, thereby reducing overall mortality. The present study aimed to evaluate pulmonary function parameters derived from spirometry (forced vital capacity [FVC], forced expiratory volume in 1 s [FEV1]), body plethysmography (residual volume [RV], total lung capacity [TLC]), and lung diffusion capacity for carbon monoxide (single-breath method [DCO-SB], alveolar-volume corrected values [DCO-VA]) as predictors of chronic hypercapnia in patients with advanced COPD.
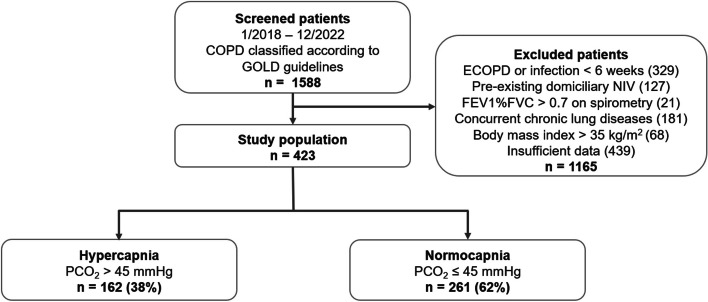
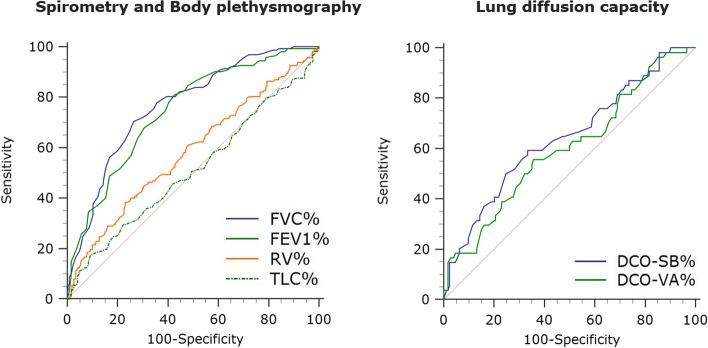
This monocentric, retrospective observational study included 423 COPD patients. Receiver operating characteristic (ROC) curve analysis and cross-validation were used to assess lung function parameters' diagnostic accuracy for predicting chronic hypercapnia, with the resulting performance expressed as area under the ROC curve (AUROC). We performed univariable and multivariable binary logistic regression analysis to determine if these parameters were independently associated with chronic hypercapnia, with probabilities reported as odds ratios [OR] with 95% confidence intervals [95%CI].
FVC% (AUROC 0.77 [95%CI 0.72-0.81], P < 0.01) and FEV1% (AURIC 0.75 [95%CI 0.70-0.79], P < 0.01) exhibited reasonable accuracy in the prediction of chronic hypercapnia, whereas lung diffusion capacity performed poorly (AUROC 0.64 [95%CI 0.58-0.71] for DCO-SB%, P < 0.01). FVC% (OR 0.95 [95%CI 0.93-0.97], P < 0.01) and FEV1% (OR 0.97 [95%CI 0.94-0.99], P = 0.029) were the only parameters associated independently with chronic hypercapnia in logistic regression analysis. FVC and FEV1 thresholds that best separated hypercapnic from normocapnic subjects reached 56% and 33% of predicted values.
Routinely collected pulmonary function parameters, particularly FVC% and FEV1%, may predict chronic hypercapnia during COPD progression.
在晚期慢性阻塞性肺疾病(COPD)中,由于严重的支气管阻塞导致肺过度充气,可能会发生高碳酸血症。无创通气(NIV)提供了旨在实现生理 PCO 水平的标准治疗,从而降低总体死亡率。本研究旨在评估从肺活量测定(用力肺活量 [FVC]、1 秒用力呼气量 [FEV1])、体描法(残气量 [RV]、总肺容量 [TLC])和一氧化碳肺扩散量(单次呼吸法 [DCO-SB]、肺泡容积校正值 [DCO-VA])得出的肺功能参数是否可预测晚期 COPD 患者的慢性高碳酸血症。
这是一项单中心、回顾性观察性研究,共纳入 423 例 COPD 患者。使用接收者操作特征(ROC)曲线分析和交叉验证来评估肺功能参数预测慢性高碳酸血症的准确性,ROC 曲线下面积(AUCROC)表示为性能指标。我们进行了单变量和多变量二元逻辑回归分析,以确定这些参数是否与慢性高碳酸血症独立相关,概率表示为比值比[OR]及其 95%置信区间[95%CI]。
FVC%(AUCROC 0.77 [95%CI 0.72-0.81],P<0.01)和 FEV1%(AUCROC 0.75 [95%CI 0.70-0.79],P<0.01)在预测慢性高碳酸血症方面具有较好的准确性,而肺扩散量的性能较差(DCO-SB%的 AUCROC 为 0.64 [95%CI 0.58-0.71],P<0.01)。FVC%(OR 0.95 [95%CI 0.93-0.97],P<0.01)和 FEV1%(OR 0.97 [95%CI 0.94-0.99],P=0.029)是逻辑回归分析中唯一与慢性高碳酸血症独立相关的参数。最佳区分高碳酸血症和正常碳酸血症患者的 FVC 和 FEV1 阈值分别达到预测值的 56%和 33%。
常规收集的肺功能参数,特别是 FVC%和 FEV1%,可能可预测 COPD 进展过程中的慢性高碳酸血症。