Pandis Dimosthenis, David Navindra, Ei-Eshmawi Ahmed, Miller Marc A, Boateng Percy, Costa Ana Claudia, Robson Philip, Trivieri Maria Giovanna, Fayad Zahi, Anyanwu Anelechi C, Adams David H
Department of Cardiovascular Surgery, Icahn School of Medicine at Mount Sinai, New York, NY.
The Icahn School of Medicine at Mount Sinai, New York, NY.
JTCVS Open. 2024 Apr 18;19:94-113. doi: 10.1016/j.xjon.2024.04.005. eCollection 2024 Jun.
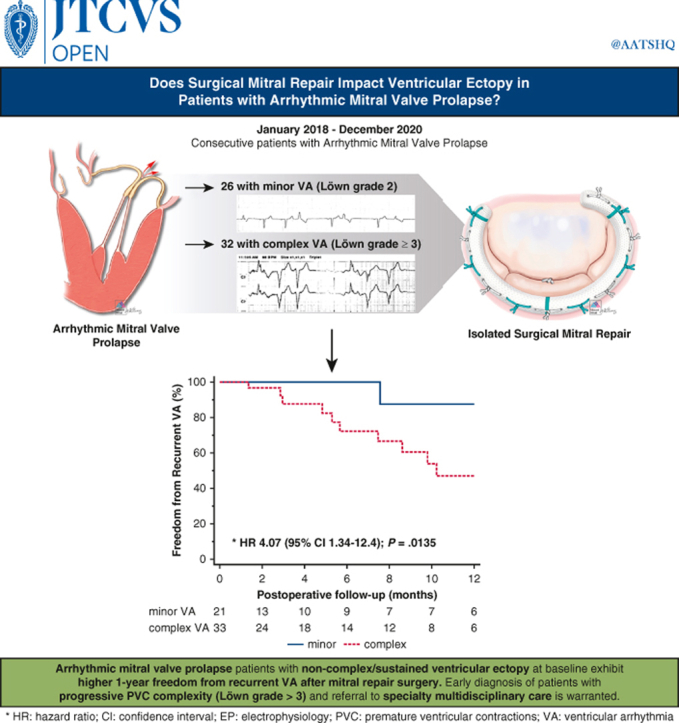
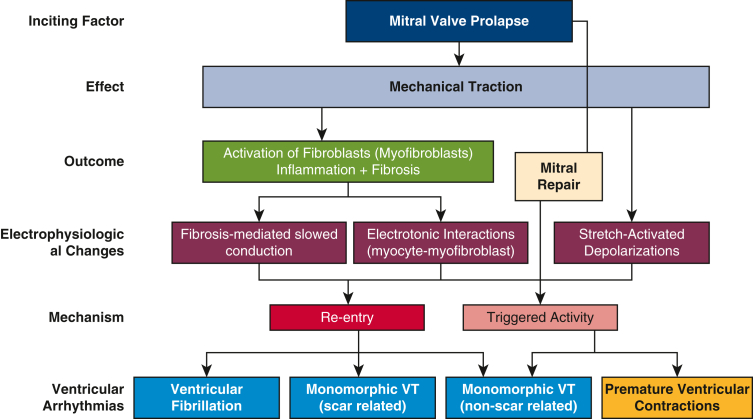
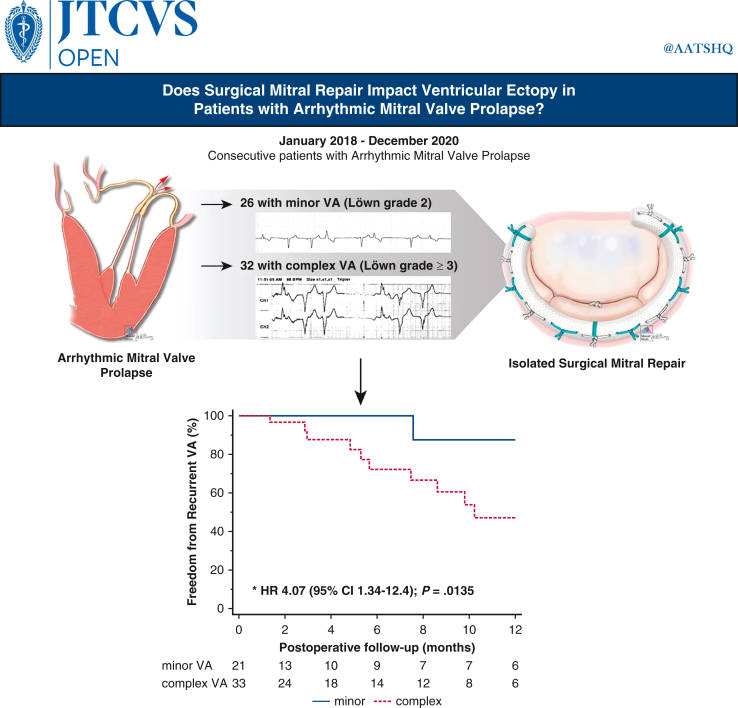
The effect of mitral valve (MV) surgery on the natural history of ventricular arrhythmia (VA) in patients with arrhythmic MV prolapse remains unknown. We sought to evaluate the cumulative incidence of VA at 1 year after surgical mitral repair.
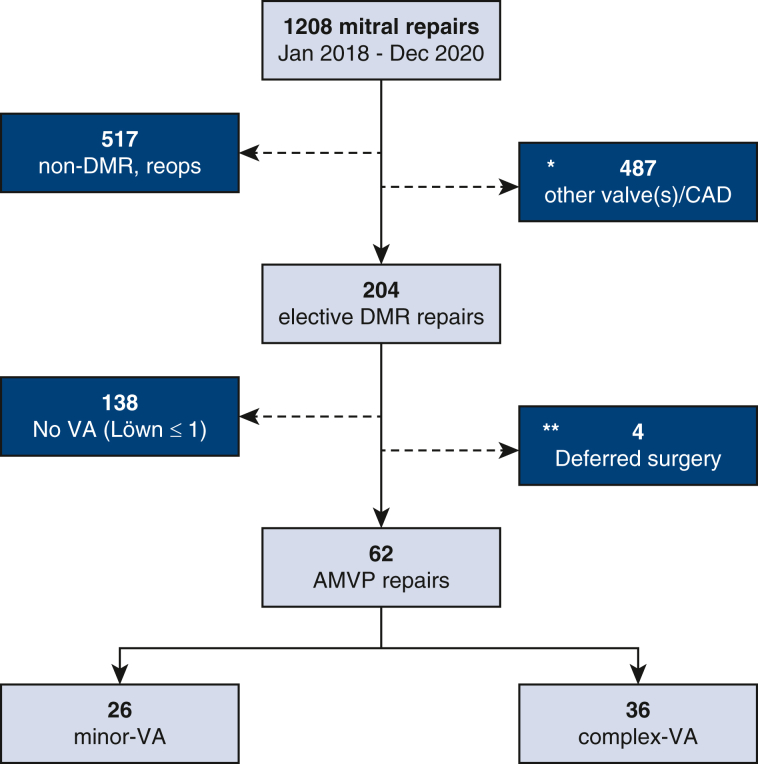
A retrospective review of progressively captured data identified 204 consecutive patients who underwent elective MV repair for significant degenerative mitral regurgitation as a first-time cardiovascular intervention in a quaternary reference center between January 2018 and December 2020. A subset of 62 consecutive patients with diagnosed arrhythmic MV prolapse was further evaluated for recurrent VA after MV repair.
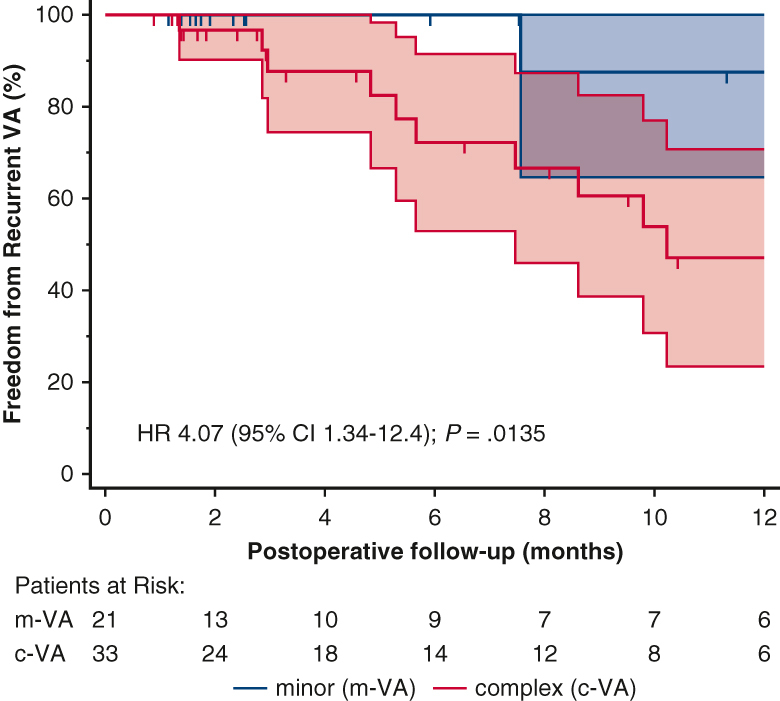
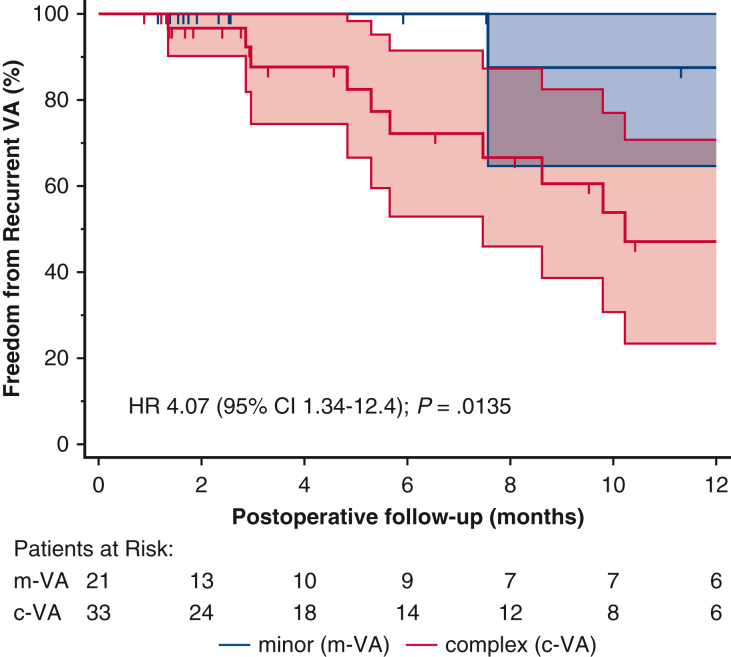
The median age was 62 years (range, 27-77 years) and 26 of 62 (41.9%) were female. The median time from initial mitral regurgitation/MV prolaspe diagnosis-to-referral was 13.8 years (interquartile range [IQR], 5.4-25) and from VA diagnosis-to-referral was 8 years (IQR, 3-10.6). Using the Lown-Wolf classification, complex VA (Lown grade ≥3) was identified in 36 of 62 patients (58%) at baseline, whereas 8 of 62 (13%) had a cardioverter/defibrillator implanted for primary (4/8) or secondary (4/8) prevention. Left ventricular myocardial scar was confirmed in 23 of 34 (68%) of patients scanned at baseline. The prevailing valve phenotype was bileaflet Barlow (59/62; 95.2%). All patients underwent surgical MV repair by the same team. Surgical repair was stabilized with an annuloplasty prosthesis (median size 36 mm [IQR, 34-38]). Concomitant procedures included tricuspid valve repair (51/62; 82.3%), cryo-maze ± left atrial appendage exclusion (14/62, 23%), and endocardial cryoablation of VA ectopy (4/62; 6.5%). The 30-day and 1-year freedom from recurrent VA were 98.4% and 75.9%, respectively. Absent VA after mitral repair was uniformly observed in patients with minor VA at baseline. Absent VA after mitral repair was uniformly observed in patients with minor VA preoperatively. Complex baseline VA was the strongest predictor of recurrent VA (hazard ratio, 10.8; 95% confidence interval, 1.4-84.2; = .024), irrespective of myocardial fibrosis.
In a series of 62 consecutive patients operated electively for arrhythmic mitral prolapse, VA remained undetected in 75.9% of patients at 1 year. Freedom from recurrent VA was greater among patients without complex VA preoperatively, whereas baseline Lown grade ≥3 was the strongest independent risk factor for recurrent VA at 1 year. These findings attest to the importance of early recognition and prompt referral of patients with mitral prolapse and progressive VA to specialty interdisciplinary care.
二尖瓣手术对心律失常性二尖瓣脱垂患者室性心律失常(VA)自然病程的影响尚不清楚。我们试图评估二尖瓣修复术后1年时VA的累积发生率。
对逐步收集的数据进行回顾性分析,确定了204例连续接受择期二尖瓣修复术治疗严重退行性二尖瓣反流的患者,这些患者于2018年1月至2020年12月在一家四级转诊中心接受首次心血管介入治疗。对62例连续诊断为心律失常性二尖瓣脱垂的患者进行了进一步评估,以观察二尖瓣修复术后VA的复发情况。
患者的中位年龄为62岁(范围27 - 77岁),62例中有26例(41.9%)为女性。从最初诊断二尖瓣反流/二尖瓣脱垂到转诊的中位时间为13.8年(四分位间距[IQR],5.4 - 25),从诊断VA到转诊的中位时间为8年(IQR,3 - 10.6)。采用洛恩 - 沃尔夫分类法,62例患者中有36例(58%)在基线时被确定为复杂性VA(洛恩分级≥3),而62例中有8例(13%)已植入心脏转复除颤器用于一级(4/8)或二级(4/8)预防。在基线时接受扫描的34例患者中有23例(68%)证实存在左心室心肌瘢痕。主要的瓣膜表型为双叶巴洛型(59/62;95.2%)。所有患者均由同一团队进行二尖瓣手术修复。手术修复通过瓣环成形假体稳定(中位尺寸36mm[IQR,34 - 38])。同期手术包括三尖瓣修复(51/62;82.3%)、冷冻迷宫术±左心耳切除术(14/62,23%)以及VA异位灶的心内膜冷冻消融术(4/62;6.5%)。VA复发率在30天和1年时分别为98.4%和75.9%。二尖瓣修复术后未出现VA在基线时为轻度VA的患者中均有一致观察到。二尖瓣修复术后未出现VA在术前为轻度VA的患者中均有一致观察到。复杂性基线VA是VA复发的最强预测因素(风险比,10.8;95%置信区间,1.4 - 84.2;P = 0.024),与心肌纤维化无关。
在一系列62例连续接受择期心律失常性二尖瓣脱垂手术的患者中,1年时75.9%的患者未检测到VA。术前无复杂性VA的患者中VA复发的情况较少,而基线洛恩分级≥3是1年时VA复发的最强独立危险因素。这些发现证明了早期识别并及时将二尖瓣脱垂和进行性VA患者转诊至专科跨学科护理的重要性。