Department of Internal Medicine, Section of Infectious Diseases, AIDS Program, Yale School of Medicine, New Haven, Connecticut, United States of America.
Harvard Combined Orthopaedic Residency Program, Boston, MA, United States of America.
PLoS One. 2024 Jul 19;19(7):e0305086. doi: 10.1371/journal.pone.0305086. eCollection 2024.
HIV incidence and mortality are increasing in Ukraine despite their reductions globally, in part due to suboptimal antiretroviral therapy (ART) coverage in key populations of people with HIV (PWH) where the epidemic is concentrated. As physicians are gatekeepers to ART prescription, stigma and discrimination barriers are understudied as a key to meeting HIV treatment targets in key populations.
A national sample (N = 204) of ART-prescribing physicians in Ukraine were surveyed between August and November 2019. Participants underwent a series of randomized, hypothetical HIV clinical scenarios and decided whether to initiate or defer (or withhold) ART. Scenarios varied based on 5 distinct CD4 counts (CD4: 17, 176, 305, 470, or 520 cells/mL) and 10 different PWH key populations. Z scores and McNemar's test for paired samples were used to assess differences between key populations and CD4 count. Feeling thermometers were used to assess stigma-related measures toward key populations among physicians.
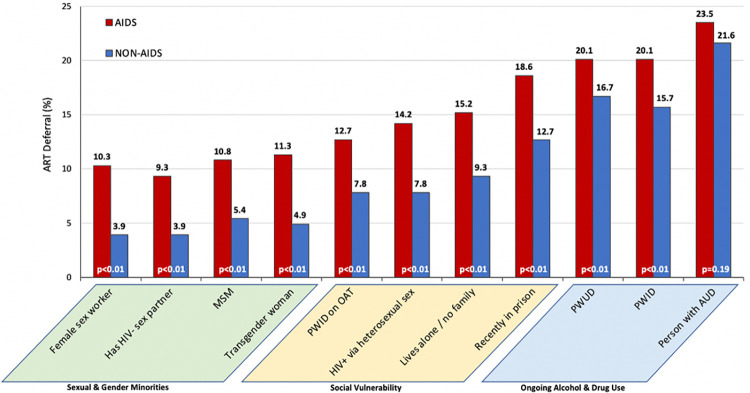
Physicians were highly experienced (mean = 19 years) HIV treaters, female (80.4%), and trained in infectious diseases (76.5%). Patients who drink alcohol (range: 21.6%-23.5%) or use (PWUD range: 16.7%-20.1%) or inject (PWID range: 15.5%-20.1%) drugs were most likely to have ART deferred, even at AIDS-defining CD4 counts. PWID maintained on methadone, however, were significantly (p<0.001) less likely to have ART deferred compared with those who were not (range: 7.8%-12.7%) on methadone. Men who have sex with men (range: 5.4%-10.8%), transgender women (range: 4.9%-11.3%), sex workers (range: 3.9%-10.3%),and having an HIV-uninfected sex partner (range: 3.9%-9.3%) had the lowest likelihood of ART deferral. Increasing levels of stigma (i.e., feeling thermometers) towards a key population was correlated with ART deferral (i.e., discrimination).
Despite international and Ukrainian guidelines recommending ART prescription for all PWH, irrespective of risk or CD4 count, ART deferral by experienced HIV experts remains high in certain key populations, especially in PWH and substance use disorders. Strategies that initiate ART immediately after diagnosis (i.e., rapid start antiretroviral therapy), independent of risk group, should be prioritized to truly mitigate the current epidemic.
尽管全球范围内艾滋病毒的发病率和死亡率都在下降,但乌克兰的这两个数据仍在上升,部分原因是艾滋病毒感染者(PLHIV)中的关键人群接受的抗逆转录病毒治疗(ART)覆盖率不足,而这些人群正是艾滋病疫情的集中地。由于医生是开具 ART 处方的把关人,因此,污名化和歧视障碍作为实现关键人群中 HIV 治疗目标的关键因素,还需要进一步研究。
2019 年 8 月至 11 月,对乌克兰 204 名开具 ART 处方的医生进行了全国性抽样调查。参与者经历了一系列随机的、假设的 HIV 临床情景,并决定是否开始、推迟(或拒绝)ART。情景根据 5 个不同的 CD4 计数(CD4:17、176、305、470 或 520 个细胞/ml)和 10 个不同的 PLHIV 关键人群而有所不同。Z 分数和配对样本 McNemar 检验用于评估关键人群与 CD4 计数之间的差异。使用感受温度计来评估医生对关键人群的与污名相关的措施。
医生在 HIV 治疗方面经验丰富(平均为 19 年),女性(80.4%),且接受过传染病培训(76.5%)。饮酒的患者(范围:21.6%-23.5%)或使用(PWUD 范围:16.7%-20.1%)或注射(PWID 范围:15.5%-20.1%)药物的患者,即使在艾滋病定义的 CD4 计数下,ART 也最有可能被推迟。然而,接受美沙酮维持治疗的注射吸毒者(范围:7.8%-12.7%)与未接受美沙酮治疗的患者相比(范围:7.8%-12.7%),ART 被推迟的可能性显著降低(p<0.001)。男男性行为者(范围:5.4%-10.8%)、跨性别女性(范围:4.9%-11.3%)、性工作者(范围:3.9%-10.3%)和有 HIV 未感染性伴侣(范围:3.9%-9.3%)的患者,ART 推迟的可能性最低。对关键人群的污名化程度(即感受温度计)越高,与 ART 推迟(即歧视)呈正相关。
尽管国际和乌克兰的指南建议为所有 PLHIV 提供 ART,无论风险或 CD4 计数如何,但在某些关键人群中,经验丰富的 HIV 专家仍然高度推迟 ART,尤其是在 PLHIV 和药物使用障碍患者中。应优先考虑在诊断后立即开始 ART(即快速启动抗逆转录病毒治疗)的策略,而不论风险群体如何,以真正减轻当前的艾滋病疫情。