Patel Tej A, Heintz Jonathan, Chen Jinbo, LaPergola Marc, Bilker Warren B, Patel Mitesh S, Arya Lily A, Patel Manali I, Bekelman Justin E, Manz Christopher R, Parikh Ravi B
University of Pennsylvania, Philadelphia.
Biostatistics Analysis Center, Perelman School of Medicine, University of Pennsylvania Health System, Philadelphia.
NEJM AI. 2024 Jun;1(6). doi: 10.1056/aioa2300228. Epub 2024 May 15.
Serious illness conversations (SICs) in the outpatient setting may improve mood and quality of life among patients with cancer and decrease aggressive end-of-life care. Interventions informed by behavioral economics may increase rates of SICs between oncology clinicians and patients, but the impact of these interventions on end-of-life spending is unknown.
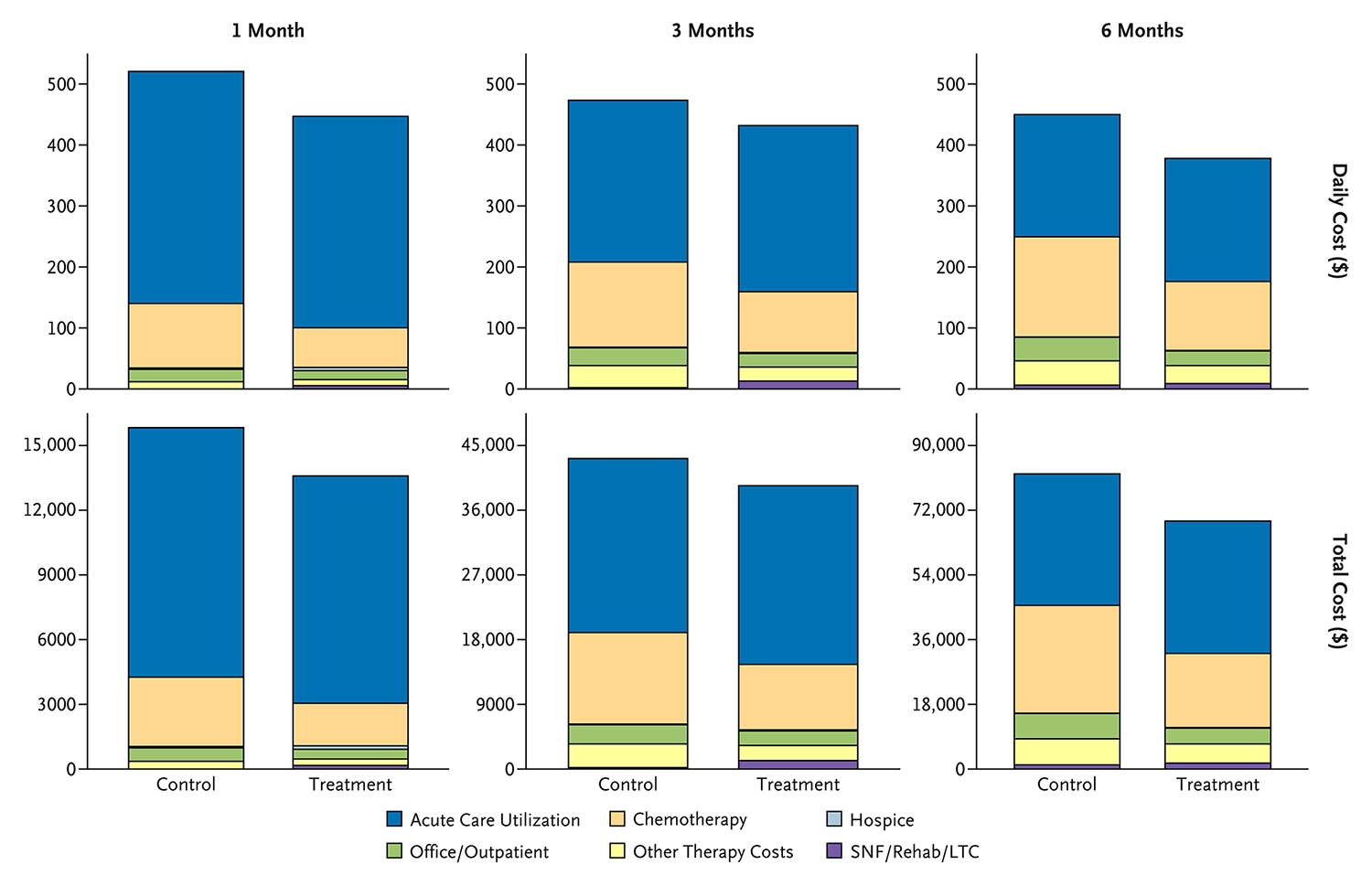
This study is a secondary analysis of a stepped-wedge cluster randomized, controlled trial that involved nine medical oncology practices and their high-risk patients at a large academic institution between June 2019 and April 2020. The study included 1187 patients who were identified by a machine-learning algorithm as high risk of 180-day mortality and who died by December 2020. The patients were randomly assigned to standard of care (controls) or to a behavioral intervention designed to increase clinician-initiated SICs. We abstracted spending - defined as inflation-adjusted costs for acute care (inpatient plus emergency room), office/outpatient care, intravenous systemic therapy, other therapy (e.g., radiation), long-term care, and hospice - from the institution's accounting system, and we captured spending at inpatient, outpatient, and pharmacy settings. To evaluate intervention impacts on spending, we used a two-part model, first using logistic regression to model zero versus nonzero spending and second using generalized linear mixed models with gamma distribution and log-link function to model daily mean spending in the last 180days of life. Models were adjusted for clinic and wedge fixed effects, and they were clustered at the oncologist level. For all patients with at least one SIC within 6 months of death, we also calculated their mean daily spending before and after SIC.
Median age at death was 68years (interquartile range, 15.5), 317 patients (27%) were Black or of ethnicities other than white, and 448 patients (38%) had an SIC. The intervention was associated with lower unadjusted mean daily spending in the last 6 months of life for the intervention group versus controls ($377.96 vs. $449.92; adjusted mean difference, -$75.33; 95% confidence interval, -$136.42 to -$14.23; P=0.02), translating to $13,747 total adjusted savings per decedent and $13 million in cumulative savings across all decedents in the intervention group. Compared with controls, patients in the intervention group incurred lower mean daily spending for systemic therapy (adjusted difference, -$44.59; P=0.001), office/outpatient care (-$9.62; P=0.001), and other therapy (-$8.65; P=0.04). The intervention was not associated with differences in end-of-life spending for acute care, long-term care, or hospice. Results were consistent for spending in the last 1 and 3 months of life and after adjusting for age, race, and ethnicity. For patients with SICs, mean daily spending decreased by $37.92 following the first SIC ($329.87 vs. $291.95).
A machine learning-based, behaviorally informed intervention to prompt SICs led to end-of-life savings among patients with cancer, driven by decreased systemic therapy and outpatient spending. (Funded by the Penn Center for Precision Medicine and the National Institutes of Health; ClinicalTrials.gov number, NCT03984773.).
门诊环境中的重病谈话(SICs)可能改善癌症患者的情绪和生活质量,并减少积极的临终关怀。基于行为经济学的干预措施可能会提高肿瘤临床医生与患者之间进行SICs的比例,但这些干预措施对临终支出的影响尚不清楚。
本研究是一项阶梯楔形整群随机对照试验的二次分析,该试验于2019年6月至2020年4月在一家大型学术机构中涉及9个医学肿瘤学实践及其高危患者。该研究纳入了1187名被机器学习算法识别为180天死亡高风险且于2020年12月前死亡的患者。患者被随机分配至标准治疗(对照组)或旨在增加临床医生发起的SICs的行为干预组。我们从该机构的会计系统中提取了支出——定义为急性护理(住院加急诊室)、门诊/门诊护理、静脉全身治疗、其他治疗(如放疗)、长期护理和临终关怀的通胀调整成本——并记录了住院、门诊和药房环境中的支出。为了评估干预对支出的影响,我们使用了一个两部分模型,首先使用逻辑回归对零支出与非零支出进行建模,其次使用具有伽马分布和对数链接函数的广义线性混合模型对生命最后180天的日均支出进行建模。模型对诊所和楔形固定效应进行了调整,并在肿瘤学家层面进行了聚类。对于所有在死亡前6个月内至少进行过一次SIC的患者,我们还计算了他们在SIC前后的日均支出。
死亡时的中位年龄为68岁(四分位间距,15.5),317名患者(27%)为黑人或非白人种族,448名患者(38%)进行了SIC。与对照组相比,干预组在生命最后6个月的未调整日均支出较低(377.96美元对449.92美元;调整后的平均差异为-75.33美元;95%置信区间,-136.42美元至-14.23美元;P=0.02),这意味着干预组每名死者的总调整后节省为13747美元,所有死者的累计节省为1300万美元。与对照组相比,干预组患者在全身治疗(调整后的差异为-44.59美元;P=0.001)、门诊/门诊护理(-9.62美元;P=0.001)和其他治疗(-8.65美元;P=0.04)方面的日均支出较低。干预与急性护理、长期护理或临终关怀的临终支出差异无关。在生命的最后1个月和3个月以及在调整年龄、种族和民族后,结果在支出方面是一致的。对于进行过SIC的患者,首次SIC后日均支出减少了37.92美元(329.87美元对291.95美元)。
一种基于机器学习、以行为学为依据促使进行SICs的干预措施,在癌症患者临终时节省了费用,这是由全身治疗和门诊支出的减少所驱动的。(由宾夕法尼亚精准医学中心和美国国立卫生研究院资助;ClinicalTrials.gov编号,NCT03984773。)