Gentzler Ryan D, Guittar John, Mitra Akash, Iams Wade T, Driessen Terri, Schwind Regina, Stein Michelle M, Kaneva Kristiyana, Hyun Seung Won, Liu Yan, Dugan Adam J, Vibat Cecile Rose T, Sangli Chithra, Freaney Jonathan, Rivers Zachary, Feliciano Josephine L, Lo Christine, Sasser Kate, Ben-Shachar Rotem, Nimeiri Halla, Patel Jyoti D, Chaudhuri Aadel A
Department of Hematology and Oncology, University of Virginia, Charlottesville, VA, USA.
Tempus AI, Inc., 600 West Chicago Avenue, Suite 510, Chicago, IL, 60654, USA.
Oncol Ther. 2024 Sep;12(3):509-524. doi: 10.1007/s40487-024-00287-2. Epub 2024 Jul 22.
A dynamic molecular biomarker that can identify early efficacy of immune checkpoint inhibitor (ICI) therapy remains an unmet clinical need. Here we evaluate if a novel circulating tumor DNA (ctDNA) assay, xM, used for treatment response monitoring (TRM), that quantifies changes in ctDNA tumor fraction (TF), can predict outcome benefits in patients treated with ICI alone or in combination with chemotherapy in a real-world (RW) cohort.
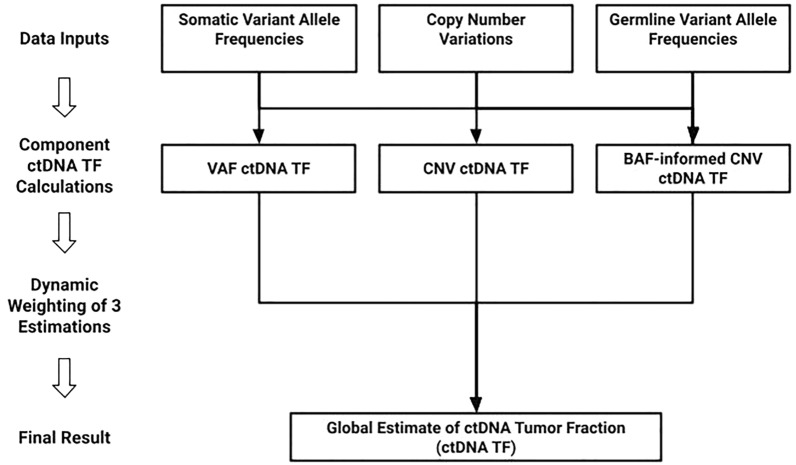
This retrospective study consisted of patients with advanced cancer from the Tempus de-identified clinical genomic database who received longitudinal liquid-based next-generation sequencing. Eligible patients had a blood sample ≤ 40 days prior to the start of ICI initiation and an on-treatment blood sample 15-180 days post ICI initiation. TF was calculated via an ensemble algorithm that utilizes TF estimates derived from variants and copy number information. Patients with molecular response (MR) were defined as patients with a ≥ 50% decrease in TF between tests. In the subset of patients with rw-imaging data between 2 and 18 weeks of ICI initiation, the predictive value of MR in addition to rw-imaging was compared to a model of rw-imaging alone.
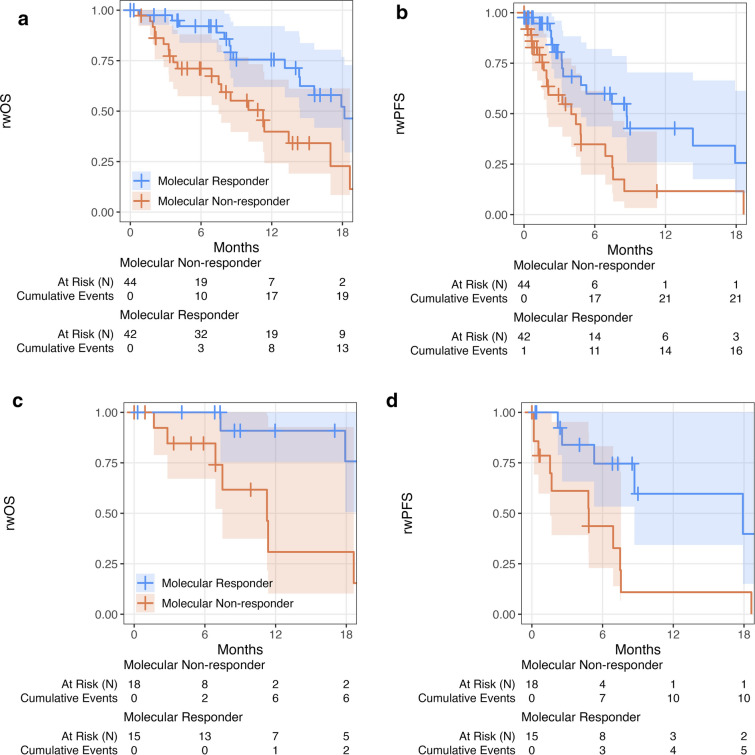
The evaluable cohort (N = 86) was composed of 14 solid cancer types. Patients received either ICI monotherapy (38.4%, N = 33) or ICI in combination with chemotherapy (61.6%, N = 53). Patients with MR had significantly longer rw-overall survival (rwOS) (hazard ratio (HR) 0.4, P = 0.004) and rw-progression free survival (rwPFS) (HR 0.4, P = 0.005) than patients with molecular non-response (nMR). Similar results were seen in the ICI monotherapy subcohort; HR 0.2, P = 0.02 for rwOS and HR 0.2, P = 0.01 for rwPFS. In the subset of patients with matched rw-imaging data (N = 51), a model incorporating both MR and rw-imaging was superior in predicting rwOS than rw-imaging alone (P = 0.02).
xM used for TRM is a novel serial quantitative TF algorithm that can be used clinically to evaluate ICI therapy efficacy.
一种能够识别免疫检查点抑制剂(ICI)治疗早期疗效的动态分子生物标志物仍是尚未满足的临床需求。在此,我们评估一种用于治疗反应监测(TRM)的新型循环肿瘤DNA(ctDNA)检测方法xM,该方法可量化ctDNA肿瘤分数(TF)的变化,能否预测在真实世界(RW)队列中接受单纯ICI治疗或联合化疗的患者的预后获益。
这项回顾性研究纳入了来自Tempus匿名临床基因组数据库的晚期癌症患者,这些患者接受了基于液体的纵向二代测序。符合条件的患者在ICI开始前≤40天有一份血样,在ICI开始后15 - 180天有一份治疗期间血样。TF通过一种整合算法计算得出,该算法利用从变异和拷贝数信息得出的TF估计值。分子反应(MR)患者定义为两次检测之间TF下降≥50%的患者。在ICI开始后2至18周有rw影像学数据的患者亚组中,将MR联合rw影像学的预测价值与单纯rw影像学模型进行比较。
可评估队列(N = 86)由14种实体癌类型组成。患者接受ICI单药治疗(38.4%,N = 33)或ICI联合化疗(61.6%,N = 53)。与分子无反应(nMR)患者相比,MR患者的rw总生存期(rwOS)显著更长(风险比(HR)0.4,P = 0.004),rw无进展生存期(rwPFS)也显著更长(HR 0.4,P = 0.005)。在ICI单药治疗亚组中也观察到类似结果;rwOS的HR为0.2,P = 0.02,rwPFS的HR为0.2,P = 0.01。在有匹配rw影像学数据的患者亚组(N = 51)中,一个包含MR和rw影像学的模型在预测rwOS方面优于单纯rw影像学(P = 0.02)。
用于TRM的xM是一种新型的连续定量TF算法,可在临床上用于评估ICI治疗疗效。