Division of Molecular Pathology, The Institute of Cancer Research, London, UK.
Unit of Biostatistics for Clinical Research, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy.
Cancer Med. 2024 Jul;13(14):e70026. doi: 10.1002/cam4.70026.
High-risk soft tissue sarcomas of the extremities and trunk wall (eSTS), as defined by the Sarculator nomogram, are more likely to benefit from (neo)adjuvant anthracycline-based therapy compared to low/intermediate-risk patients. The biology underpinning these differential treatment outcomes remain unknown.
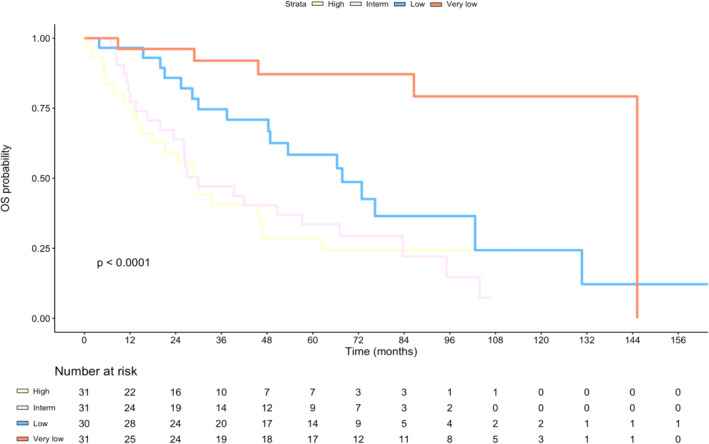
We analysed proteomic profiles and clinical outcomes of 123 eSTS patients. A Cox model for overall survival including the Sarculator was fitted to individual data to define four risk groups. A DNA replication protein signature-Sarcoma Proteomic Module 6 (SPM6) was evaluated for association with clinicopathological factors and risk groups. SPM6 was added as a covariate together with Sarculator in a multivariable Cox model to assess improvement in prognostic risk stratification.
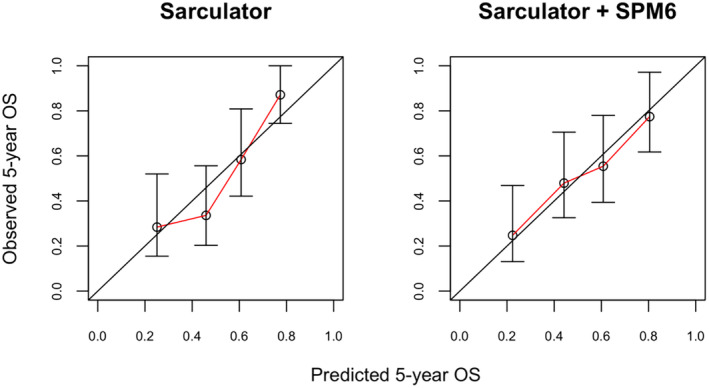
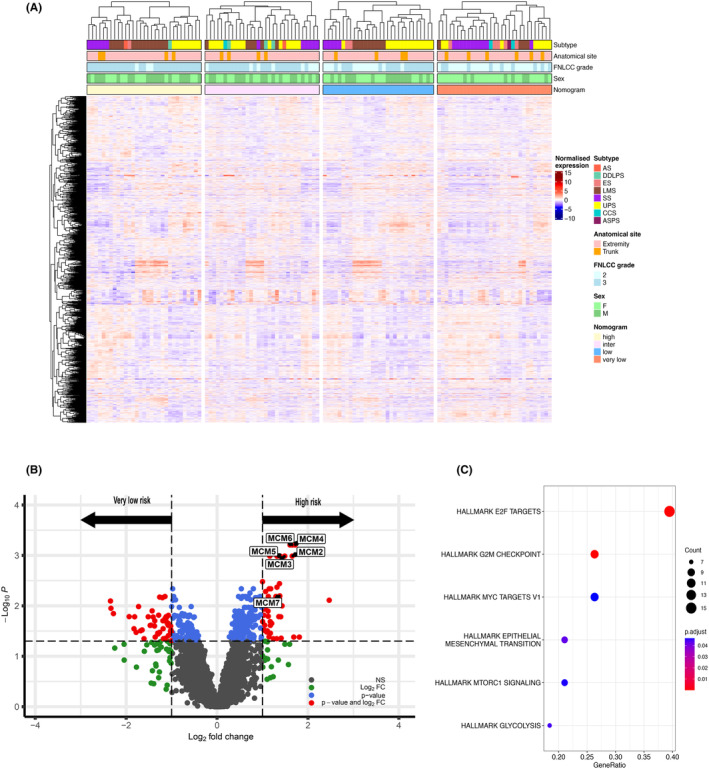
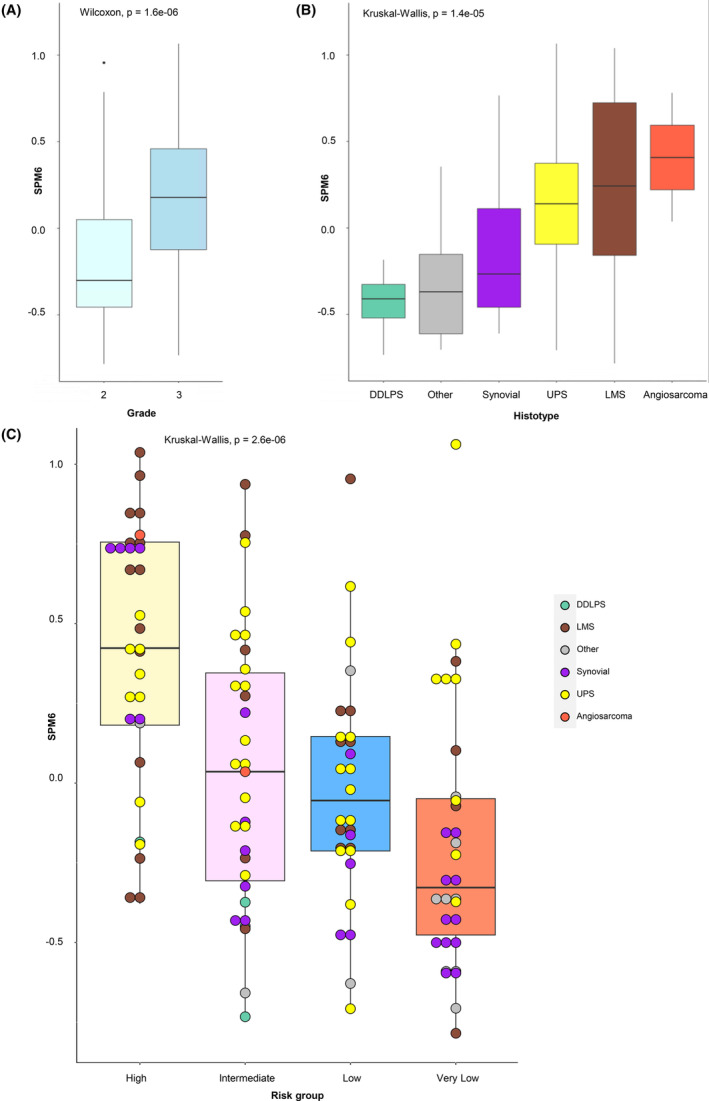
DNA replication and cell cycle proteins were upregulated in high-risk versus very low-risk patients. Evaluation of the functional effects of CRISPR-Cas9 gene knockdown of proteins enriched in high-risk patients using the cancer cell line encyclopaedia database identified candidate drug targets. SPM6 was significantly associated with tumour malignancy grade (p = 1.6e-06), histology (p = 1.4e-05) and risk groups (p = 2.6e-06). Cox model analysis showed that SPM6 substantially contributed to a better calibration of the Sarculator nomogram (Index of Prediction Accuracy = 0.109 for Sarculator alone versus 0.165 for Sarculator + SPM6).
Risk stratification of patient with STS is defined by distinct biological pathways across a range of cancer hallmarks. Incorporation of SPM6 protein signature improves prognostic risk stratification of the Sarculator nomogram. This study highlights the utility of integrating protein signatures for the development of next-generation nomograms.
根据 Sarculator 风险预测图定义的肢体和躯干壁高危软组织肉瘤(eSTS)与低/中危患者相比,更有可能从(新)辅助蒽环类药物治疗中获益。支持这些差异化治疗结果的生物学机制尚不清楚。
我们分析了 123 例 eSTS 患者的蛋白质组学特征和临床结局。使用包括 Sarculator 的 Cox 模型对个体数据进行整体生存分析,以定义四个风险组。评估与临床病理因素和风险组相关的 DNA 复制蛋白标志物-肉瘤蛋白质组模块 6(SPM6)。将 SPM6 与 Sarculator 一起作为协变量添加到多变量 Cox 模型中,以评估其对预后风险分层的改善作用。
与极低危患者相比,高危患者的 DNA 复制和细胞周期蛋白上调。使用癌症细胞系百科全书数据库评估 CRISPR-Cas9 基因敲低富含高危患者的蛋白质的功能效应,确定了候选药物靶点。SPM6 与肿瘤恶性程度(p=1.6e-06)、组织学(p=1.4e-05)和风险组(p=2.6e-06)显著相关。Cox 模型分析表明,SPM6 极大地提高了 Sarculator 预测图的校准度(Sarculator 单独的预测准确性指数为 0.109,而 Sarculator+SPM6 的预测准确性指数为 0.165)。
STS 患者的风险分层由一系列癌症特征的不同生物学途径定义。纳入 SPM6 蛋白特征可改善 Sarculator 预测图的预后风险分层。本研究强调了整合蛋白质特征用于开发下一代预测图的实用性。