Department of Oncology, National Taiwan University Hospital, Taipei, Taiwan.
Department of Surgery, National Taiwan University, Taipei, Taiwan.
Cancer Med. 2024 Jul;13(14):e70005. doi: 10.1002/cam4.70005.
Due to cardiotoxicity concerns, the concurrent use of epirubicin and trastuzumab has not been fully studied. This study aimed to examine the cardiotoxicity and pathological complete response (pCR) rate associated with the concurrent regimens in patients with human epidermal growth factor receptor 2 (HER2)-positive early breast cancer (EBC).
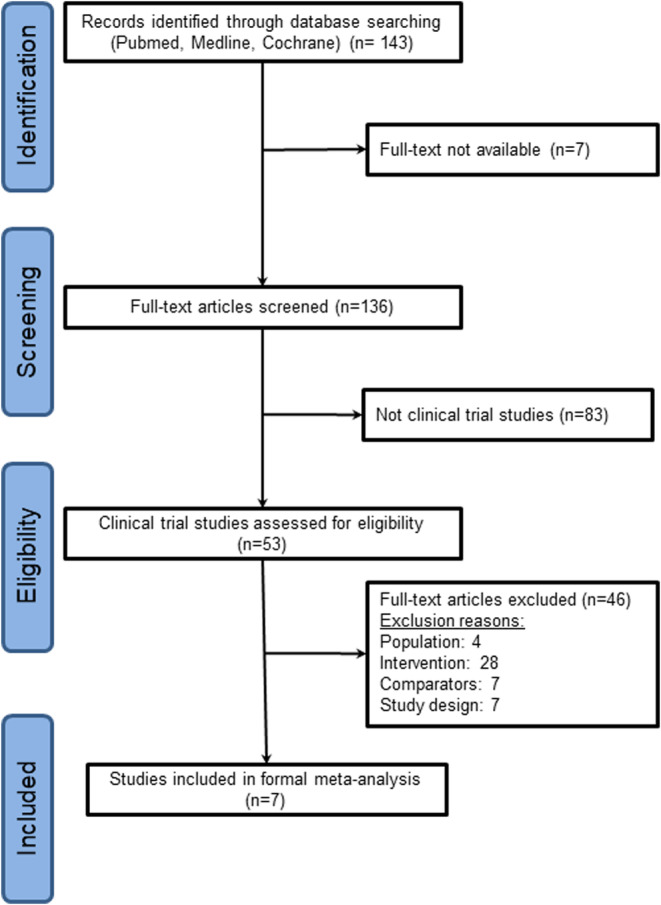
We conducted a systematic search for relevant literature in the NCBI/PubMed, the Cochrane database, and international conference abstracts for phase II or III randomized controlled trials between January 1, 2000, and February 28, 2021, focusing on the concurrent regimens in patients with HER2-positive EBC. To compare the risk of cardiotoxicity and the odds of the pCR rate, we performed linear meta-regression analyses to investigate the effects of multiple covariates.
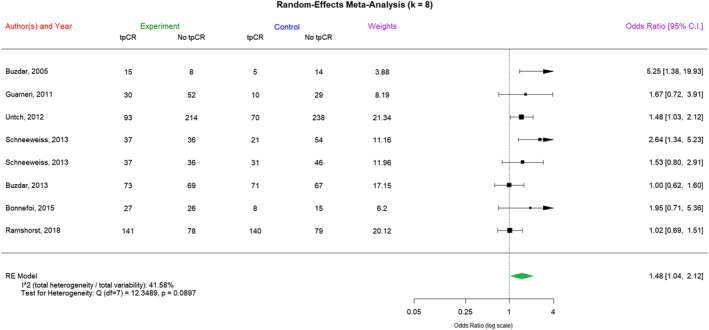
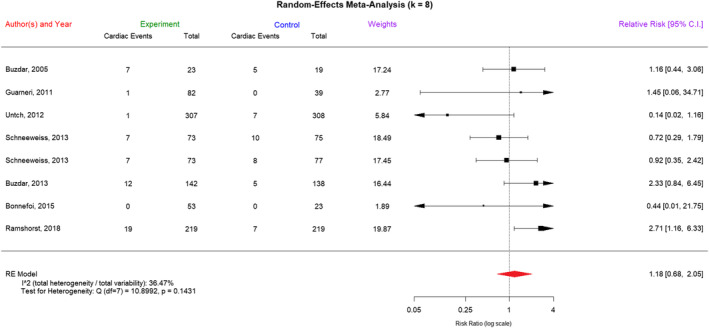
We analyzed 7 neoadjuvant trials involving the concurrent use of epirubicin and trastuzumab with 1797 patients. The median cumulative dose of epirubicin used was 300 mg/m, with a total of 96 reported adverse cardiac events. The concurrent regimens did not result in a significant increase in cardiotoxicity compared to nonconcurrent regimens (risk ratio [RR] = 1.18, 95% confidence interval [CI] = 0.68-2.05). Compared with nonconcurrent or non-anthracycline-containing regimens, concurrent regimens were associated with a significant increase in the pCR rate (odds ratio = 1.48, 95% CI = 1.04-2.12). The linear fixed-effects meta-regression analysis indicated that in trials including more patients with hormone receptor-positive EBC, the RR of cardiotoxicity significantly increased with concurrent regimens, and the pCR rate became less significant.
The combination of trastuzumab and a low dose of epirubicin positively impacted the pCR rate without a significant increase in cardiotoxicity. We recommend exploring concurrent regimens for HR-negative, HER2-positive tumors to enhance pCR rates, with caution advised for HR-positive tumors due to potential cardiotoxicity.
由于心脏毒性的担忧,表柔比星和曲妥珠单抗的联合使用尚未得到充分研究。本研究旨在探讨曲妥珠单抗联合表柔比星方案在人表皮生长因子受体 2(HER2)阳性早期乳腺癌(EBC)患者中的心脏毒性和病理完全缓解(pCR)率。
我们对 2000 年 1 月 1 日至 2021 年 2 月 28 日期间的 NCBI/PubMed、Cochrane 数据库和国际会议摘要中有关 HER2 阳性 EBC 患者的曲妥珠单抗联合表柔比星方案的 II 期或 III 期随机对照试验进行了系统搜索。为了比较心脏毒性风险和 pCR 率的比值比,我们进行了线性荟萃回归分析,以研究多个协变量的影响。
我们分析了 7 项新辅助治疗试验,共纳入 1797 例患者,采用曲妥珠单抗联合表柔比星方案。使用的表柔比星累积剂量中位数为 300mg/m2,共报告了 96 例不良心脏事件。与非联合方案相比,联合方案并未导致心脏毒性显著增加(风险比[RR] = 1.18,95%置信区间[CI] = 0.68-2.05)。与非联合或非蒽环类药物方案相比,联合方案与 pCR 率显著升高相关(比值比[OR] = 1.48,95%CI = 1.04-2.12)。线性固定效应荟萃回归分析表明,在纳入更多激素受体阳性 EBC 患者的试验中,联合方案的心脏毒性 RR 显著增加,而 pCR 率变得不那么显著。
曲妥珠单抗联合低剂量表柔比星方案显著提高了 pCR 率,且不增加心脏毒性。我们建议探索曲妥珠单抗联合表柔比星方案用于 HR 阴性、HER2 阳性肿瘤,以提高 pCR 率,但对于 HR 阳性肿瘤,应谨慎使用,因为可能存在心脏毒性。