Khandelwal Priyanka, Hofstetter Jonas, Azukaitis Karolis, Bayazit Aysun, Doyon Anke, Duzova Ali, Canpolat Nur, Bulut Ipek Kaplan, Obryck Lukasz, Ranchin Bruno, Paripovic Dusan, Bakkaloglu Sevcan, Alpay Harika, Arbeiter Klaus, Litwin Mieczyslaw, Zaloszyc Ariane, Paglialonga Fabio, Borzych-Dużałka Dagmara, Schmitt Claus Peter, Melk Anette, Querfeld Uwe, Schaefer Franz, Shroff Rukshana
Division of Pediatric Nephrology, UCL Great Ormond Street Hospital and Institute of Child Health, London, UK.
Center for Pediatrics and Adolescent Medicine, University Hospital Heidelberg, Heidelberg, Germany.
EClinicalMedicine. 2024 Jul 3;74:102708. doi: 10.1016/j.eclinm.2024.102708. eCollection 2024 Aug.
Despite significant cardiovascular (CV) morbidity in children on dialysis and after kidney transplantation, data on the evolution of CV damage in children with chronic kidney disease (CKD) approaching kidney replacement therapy (KRT) is unknown.
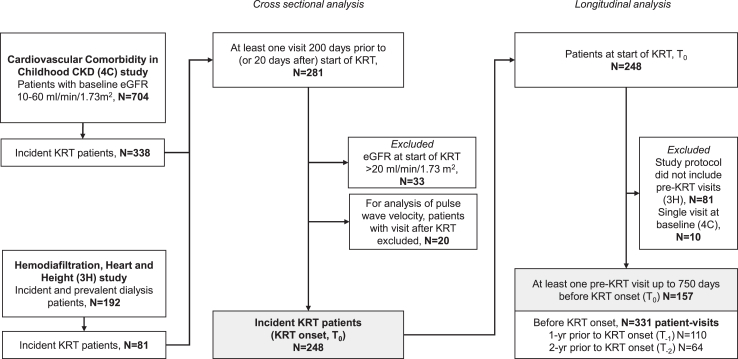
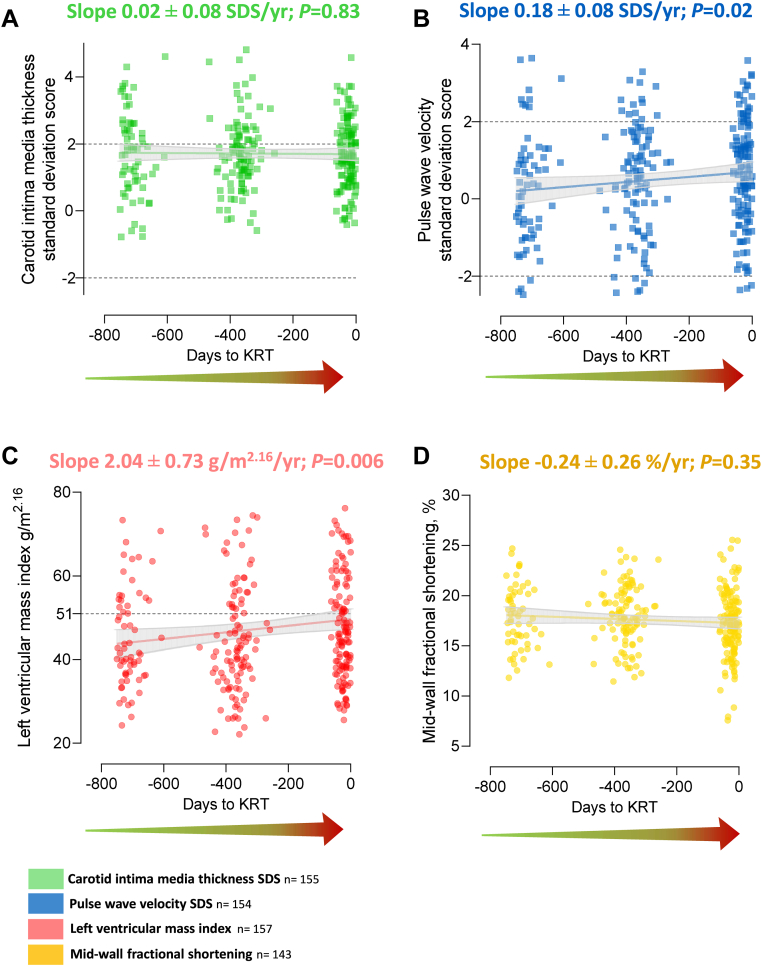
The burden, progression, and predictors of CV damage before KRT onset were explored in two prospective multicenter cohorts from Europe and Canada: Cardiovascular Comorbidity in Children with CKD (4C) and Haemodiafiltration, Heart and Height (3H) studies, conducted from 2009-19 and 2013-16, respectively. CV damage and risk factors were evaluated (i) cross sectionally at KRT-start (n = 248), and (ii) longitudinally over the 2-years preceding KRT start (n = 157; 331 patient-visits). Longitudinal analyses with mixed-effects models estimated associations of modifiable CV risk factors with change in carotid intima-media thickness (cIMT) standard deviation score (SDS), pulse wave velocity (PWV-SDS), left ventricular (LV) mass and systolic dysfunction.
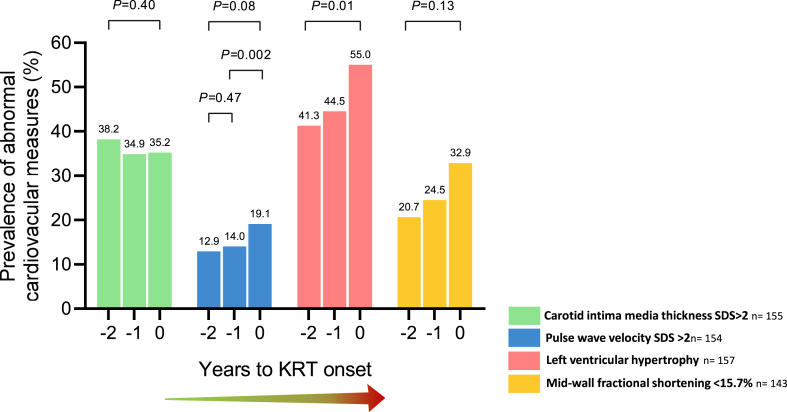
248 patients, age 14.3 (12.2, 16.2) years were evaluated at median 35 (28-114) days before KRT start. Elevated cIMT-SDS and PWV-SDS were present in 43% and 25%, and LV hypertrophy and systolic dysfunction in 49% and 33%. Aortic stiffness and LV hypertrophy significantly increased, especially in the year before KRT start (adjusted odds ratio, OR 0.33, = 0.002 and OR 0.54, = 0.01, respectively). 79% of children had >3 modifiable CV risk factors at KRT onset. Diastolic BP and BMI were strongly associated with a linear increase in all CV measures. After controlling for CV risk factors, the time to KRT onset no longer predicted the burden of CV damage.
This comprehensive CV evaluation shows the progressive accrual of modifiable risk factors and a high burden of CV damage in the years preceding KRT onset. CV damage in the pre-KRT period is preventable.
Supported by EU4Health Programme (101085068) and Kidney Research UK (RP39/2013).
尽管接受透析的儿童和肾移植后儿童存在显著的心血管(CV)疾病,但慢性肾脏病(CKD)患儿在接近肾脏替代治疗(KRT)时CV损害的演变数据尚不清楚。
在欧洲和加拿大的两个前瞻性多中心队列中探索KRT开始前CV损害的负担、进展和预测因素:分别于2009 - 19年和2013 - 16年进行的CKD患儿心血管合并症(4C)研究和血液透析滤过、心脏与身高(3H)研究。对CV损害和危险因素进行了评估:(i)在KRT开始时进行横断面评估(n = 248),以及(ii)在KRT开始前的2年中进行纵向评估(n = 157;331次患者就诊)。使用混合效应模型进行纵向分析,估计可改变的CV危险因素与颈动脉内膜中层厚度(cIMT)标准差评分(SDS)、脉搏波速度(PWV - SDS)、左心室(LV)质量和收缩功能障碍变化之间的关联。
在KRT开始前的中位数35(28 - 114)天对248例年龄为14.3(12.2,16.2)岁的患者进行了评估。cIMT - SDS升高和PWV - SDS升高的患者分别占43%和25%,LV肥厚和收缩功能障碍的患者分别占49%和33%。主动脉僵硬度和LV肥厚显著增加,尤其是在KRT开始前的一年(调整后的优势比,OR分别为0.33,P = 0.002和OR 0.54,P = 0.01)。79%的儿童在KRT开始时有超过3个可改变的CV危险因素。舒张压和BMI与所有CV指标的线性增加密切相关。在控制了CV危险因素后,KRT开始的时间不再预测CV损害的负担。
这项全面的CV评估显示,在KRT开始前的几年中,可改变的危险因素逐渐累积,CV损害负担较高。KRT前期的CV损害是可预防的。
由欧盟健康计划(101085068)和英国肾脏研究(RP39/2013)资助。