Huang Jialing, Ali Towhid, Feldman David M, Theise Neil D
Department of Pathology, Geisinger Medical Center, Geisinger Commonwealth School of Medicine, 100 N. Academy Ave, Danville, PA 17822, USA.
Department of Radiology, Geisinger Medical Center, Geisinger Commonwealth School of Medicine, 100 N. Academy Ave, Danville, PA 17822, USA.
Diagnostics (Basel). 2024 Jul 9;14(14):1473. doi: 10.3390/diagnostics14141473.
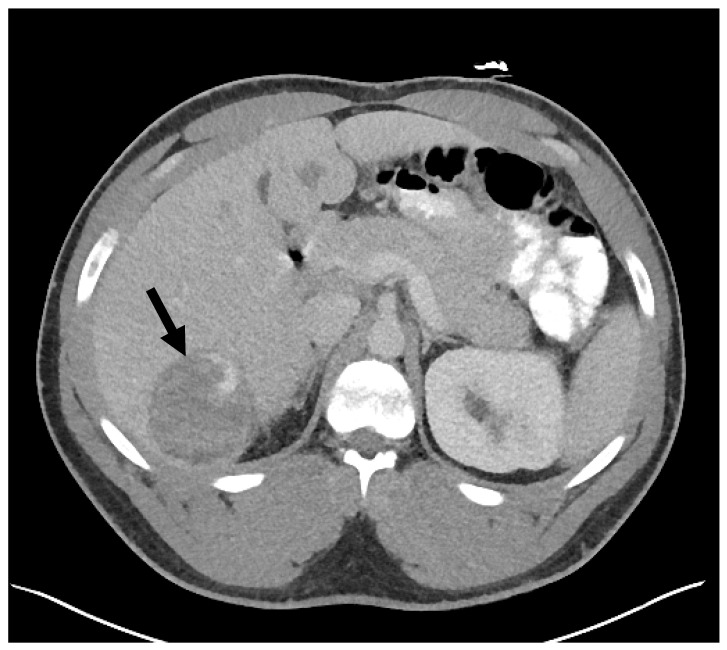
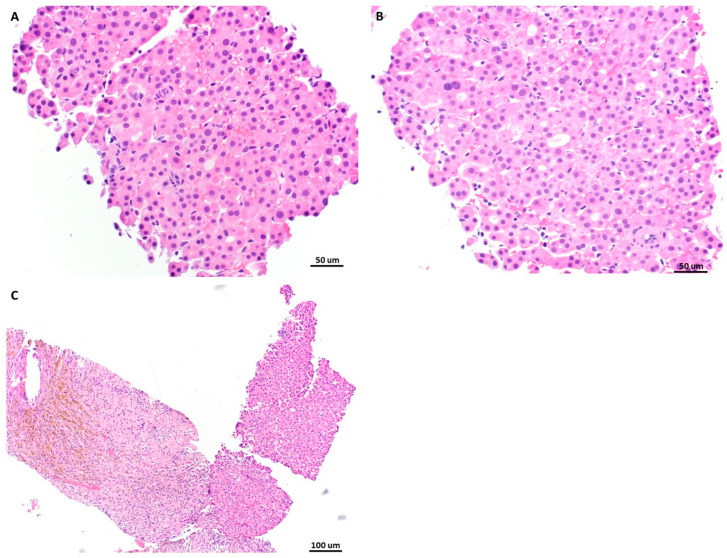
Androgens have long been recognized as oncogenic agents. They can induce both benign and malignant hepatocellular neoplasms, including hepatocellular adenoma (HCA) and hepatocellular carcinoma, though the underlying mechanisms remain unclear. Androgen-induced liver tumors are most often solitary and clinically silent. Herein, we reported an androgen-induced HCA complicated by spontaneous rupture. The patient was a 24-year-old male presenting with fatigue, diminished libido, radiology-diagnosed hepatocellular adenomatosis for 3 years, and sudden-onset, severe, sharp, constant abdominal pain for one day. He used Aveed (testosterone undecanoate injection) from age 17 and completely stopped one year before his presentation. A physical exam showed touch pain and voluntary guarding in the right upper quadrant of the abdomen. An abdominal CT angiogram demonstrated multiple probable HCAs, with active hemorrhage of the largest one (6.6 × 6.2 × 5.1 cm) accompanied by large-volume hemoperitoneum. After being stabilized by a massive transfusion protocol and interventional embolization, he underwent a percutaneous liver core biopsy. The biopsy specimen displayed atypical hepatocytes forming dense cords and pseudoglands. The lesional cells diffusely stained β-catenin in nuclei and glutamine synthetase in cytoplasm. Compared to normal hepatocytes from control tissue, the tumor cells were positive for nuclear AR (androgen receptor) expression but had no increased EZH2 (Enhancer of Zeste 2 Polycomb Repressive Complex 2 Subunit) protein expression. The case indicated that androgen-induced hepatocellular neoplasms should be included in the differential diagnosis of acute abdomen.
长期以来,雄激素一直被认为是致癌物质。它们可诱发良性和恶性肝细胞肿瘤,包括肝细胞腺瘤(HCA)和肝细胞癌,但其潜在机制尚不清楚。雄激素诱导的肝肿瘤通常为单发,临床上无明显症状。在此,我们报告一例雄激素诱导的HCA并发自发性破裂。患者为一名24岁男性,表现为疲劳、性欲减退,经影像学诊断为肝细胞腺瘤病3年,突发剧烈、尖锐、持续性腹痛1天。他从17岁开始使用Aveed(十一酸睾酮注射液),在就诊前一年完全停药。体格检查显示腹部右上象限有压痛和自主肌卫。腹部CT血管造影显示多个可能的HCA,最大的一个(6.6×6.2×5.1 cm)有活动性出血,并伴有大量腹腔积血。在通过大量输血方案和介入栓塞稳定病情后,他接受了经皮肝穿刺活检。活检标本显示非典型肝细胞形成致密索状和假腺管。病变细胞在细胞核中弥漫性染色β-连环蛋白,在细胞质中染色谷氨酰胺合成酶。与对照组织的正常肝细胞相比,肿瘤细胞的核雄激素受体(AR)表达呈阳性,但EZH2(zeste 2增强子多梳抑制复合体2亚基)蛋白表达未增加。该病例表明,雄激素诱导的肝细胞肿瘤应纳入急腹症的鉴别诊断。