Reid Michal M, Amja Jack J, Riestra Guiance Irene T, Andani Rupesh R, Vierkant Robert A, Goyal Amit, Reisenauer Janani S
Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN.
Division of Pulmonary, Critical Care, and Sleep Medicine, University of Kansas Medical Center, Kansas City, KS.
Mayo Clin Proc Innov Qual Outcomes. 2024 Jul 3;8(4):375-383. doi: 10.1016/j.mayocpiqo.2024.05.005. eCollection 2024 Aug.
To perform a retrospective, multicenter, external validation of the Cleveland Clinic malignancy probability prediction model for incidental pulmonary nodules.
From July 1, 2022, to May 31, 2023, we identified 296 patients who underwent tissue acquisition at Mayo Clinic (MC) (n=198) and Loyola University Medical Center (n=98) with histopathology indicating malignant (n=195) or benign (n=101). Data was collected at initial radiographic identification (point 1) and at the time of intervention (point 2). Point 3 represented the most recent data. The areas under the receiver operating characteristics were calculated for each model per time point. Calibration was evaluated by comparing the predicted and observed rates of malignancy.
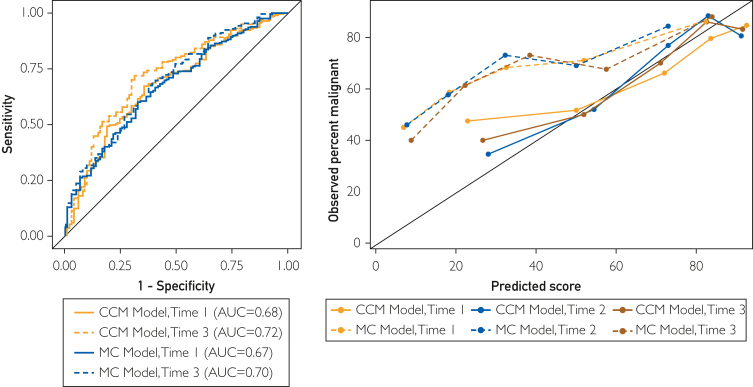
The areas under the receiver operating characteristics at time points 1, 2, and 3 for the MC model were 0.67 (95% CI, 0.61-0.74), 0.67 (95% CI, 0.58-0.77), and 0.70 (95% CI, 0.63-0.76), respectively. The Cleveland Clinic model (CCM) was 0.68 (95% CI, 0.61-0.74), 0.75 (95% CI, 0.65-0.84), and 0.72 (95% CI, 0.66-0.78), respectively. The mean ± SD estimated probability for malignant pulmonary nodules (PNs) at time points 1, 2, and 3 for the CCM was 64.2±25.9, 65.8±24.0, and 64.7±24.4, which resembled the overall proportion of malignant PNs (66%). The mean estimated probability of malignancy for the MC model at each time point was 38.3±27.4, 36.2±24.4, and 42.1±27.3, substantially lower than the observed proportion of malignancies.
The CCM found discrimination similar to its internal validation and good calibration. The CCM can be used to augment clinical and shared decision-making when evaluating high-risk PNs.
对克利夫兰诊所偶然发现的肺结节恶性概率预测模型进行回顾性、多中心外部验证。
从2022年7月1日至2023年5月31日,我们确定了296例在梅奥诊所(MC)(n = 198)和洛约拉大学医学中心(n = 98)接受组织采集的患者,其组织病理学显示为恶性(n = 195)或良性(n = 101)。在初始影像学识别时(时间点1)和干预时(时间点2)收集数据。时间点3代表最新数据。计算每个模型在每个时间点的受试者操作特征曲线下面积。通过比较预测的和观察到的恶性率来评估校准情况。
MC模型在时间点1、2和3的受试者操作特征曲线下面积分别为0.67(95%CI,0.61 - 0.74)、0.67(95%CI,0.58 - 0.77)和0.70(95%CI,0.63 - 0.76)。克利夫兰诊所模型(CCM)分别为0.68(95%CI,0.61 - 0.74)、0.75(95%CI,0.65 - 0.84)和0.72(95%CI,0.66 - 0.78)。CCM在时间点1、2和3时,恶性肺结节(PNs)的平均±标准差估计概率分别为64.2±25.9、65.8±24.0和64.7±24.4,与恶性PNs的总体比例(66%)相似。MC模型在每个时间点的恶性平均估计概率分别为38.3±27.4、36.2±24.4和42.1±27.3,显著低于观察到的恶性比例。
CCM的区分能力与其内部验证相似,且校准良好。在评估高危PNs时,CCM可用于加强临床和共同决策。