Kim Hong-Ju, Yang Pil-Sung, Kim Daehoon, Sung Jung-Hoon, Jang Eunsun, Yu Hee Tae, Kim Tae-Hoon, Pak Hui-Nam, Lee Moon-Hyoung, Joung Boyoung
Division of Cardiology, Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University College of Medicine, 03722 Seoul, Republic of Korea.
Department of Cardiology, CHA Bundang Medical Center, CHA University, 13496 Seongnam, Republic of Korea.
Rev Cardiovasc Med. 2024 May 11;25(5):164. doi: 10.31083/j.rcm2505164. eCollection 2024 May.
Polypharmacy is commonly observed in atrial fibrillation (AF) and is associated with poorer clinical outcomes. Our study aimed to elucidate the polypharmacy prevalence, its associated risk factors, and its relationship with adverse clinical outcomes using a 'real-world' database.
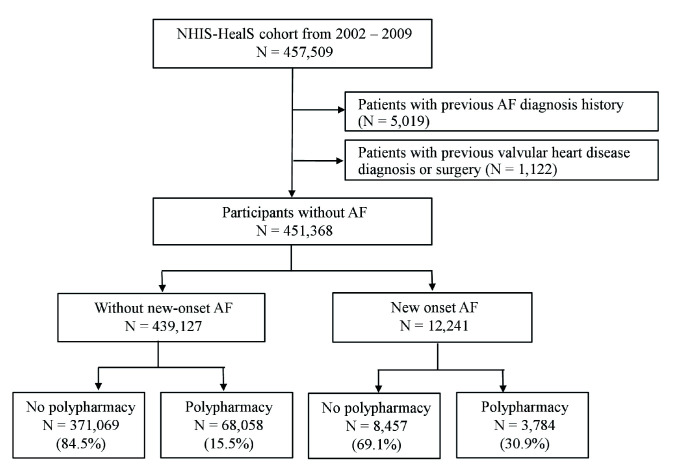
This study included 451,368 subjects without prior history of AF (median age, 54 [interquartile range, 48.0-63.0] years; 207,748 [46.0%] female) from the Korea National Health Insurance Service-Health Screening (NHIS-HealS) database between 2002 and 2013. All concomitant medications prescribed were collected, and the intake of five or more concomitant drugs was defined as polypharmacy. During the follow-up, all-cause death, major bleeding events, transient ischemic attack (TIA) or ischemic stroke, and admission due to worsened heart failure were recorded.
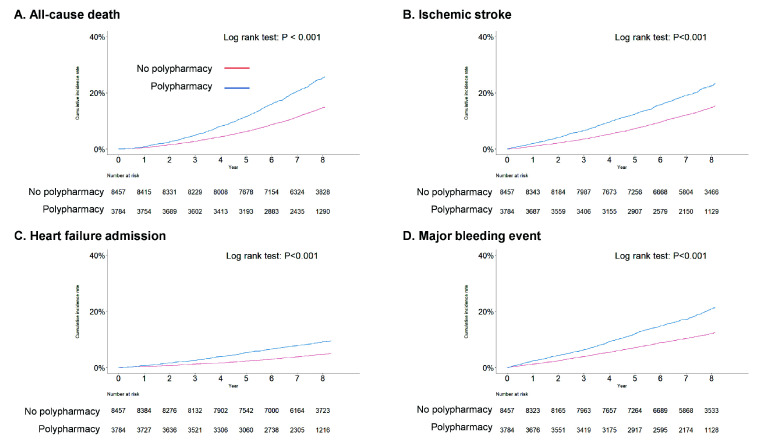
Based on up to 7.7 (6.8-8.3) years of follow-up and 768,306 person-years, there were 12,241 cases of new-onset AF identified. Among patients with new-onset AF (40.0% females, median age 63.0 [54.0-70.0] years), the polypharmacy prevalence was 30.9% (3784). For newly diagnosed AF, factors, such as advanced age (with each increase of 10 years, odds ratios (OR) 1.32, 95% confidence interval (CI) 1.26-1.40), hypertension (OR 4.00, 95% CI 3.62-4.43), diabetes mellitus (OR 3.25, 95% CI 2.86-3.70), chronic obstructive pulmonary disease (COPD) (OR 3.00, 95% CI 2.51-3.57), TIA/ischemic stroke (OR 2.36, 95% CI 2.03-2.73), dementia history (OR 2.30, 95% CI 1.06-4.98), end-stage renal disease (ESRD) or chronic kidney disease (CKD) (OR 1.97, 95% CI 1.38-2.82), and heart failure (OR 1.95, 95% CI 1.69-2.26), were found to be independently correlated with the incidence of polypharmacy. Polypharmacy significantly increased the incidence and risk of major bleeding (adjusted hazard ratio (aHR) 1.26, 95% CI 1.12-1.41). The study observed a statistically significant increase in the incidence of all-cause mortality, however, the risk for all-cause mortality elevated but did not show significance (aHR 1.11, 95% CI 0.99-1.24). The risk of stroke and admission for heart failure did not change with polypharmacy.
In our investigation using data from a nationwide database, polypharmacy was widespread in new-onset AF population and was related to major bleeding events. However, polypharmacy does not serve as an independent risk factor for adverse outcomes, with exception of major bleeding event. For AF patients, ensuring tailored medication for comorbidities as well as reducing polypharmacy are essential considerations.
多重用药在心房颤动(AF)患者中普遍存在,且与较差的临床结局相关。我们的研究旨在利用一个“真实世界”数据库阐明多重用药的患病率、相关危险因素及其与不良临床结局的关系。
本研究纳入了2002年至2013年间韩国国民健康保险服务健康筛查(NHIS-HealS)数据库中451368例无AF病史的受试者(中位年龄54岁[四分位间距,48.0 - 63.0岁];207748例[46.0%]为女性)。收集所有开具的合并用药,将服用五种或更多种合并药物定义为多重用药。在随访期间,记录全因死亡、重大出血事件、短暂性脑缺血发作(TIA)或缺血性卒中以及因心力衰竭加重而住院的情况。
基于长达7.7(6.8 - 8.3)年的随访和768306人年,共识别出12241例新发AF病例。在新发AF患者中(40.0%为女性,中位年龄63.0岁[54.0 - 70.0岁]),多重用药患病率为30.9%(3784例)。对于新诊断的AF,发现高龄(每增加10岁,比值比(OR)1.32,95%置信区间(CI)1.26 - 1.40)、高血压(OR 4.00,95% CI 3.62 - 4.43)、糖尿病(OR 3.25,95% CI 2.86 - 3.70)、慢性阻塞性肺疾病(COPD)(OR 3.00,95% CI 2.51 - 3.57)、TIA/缺血性卒中(OR 2.36,95% CI 2.03 - 2.73)、痴呆病史(OR 2.30,95% CI 1.06 - 4.98)、终末期肾病(ESRD)或慢性肾脏病(CKD)(OR 1.97,95% CI 1.38 - 2.82)以及心力衰竭(OR 1.95,95% CI 1.69 - 2.26)等因素与多重用药的发生率独立相关。多重用药显著增加了重大出血的发生率和风险(调整后风险比(aHR)1.26,95% CI 1.12 - 1.41)。该研究观察到全因死亡率的发生率有统计学显著增加,然而,全因死亡风险升高但未显示出显著性(aHR 1.11,95% CI 0.99 - 1.24)。卒中风险和因心力衰竭住院风险并未因多重用药而改变。
在我们使用全国性数据库数据进行的调查中,多重用药在新发AF人群中普遍存在,且与重大出血事件相关。然而,除重大出血事件外,多重用药并非不良结局的独立危险因素。对于AF患者,确保针对合并症的个体化用药以及减少多重用药是至关重要的考虑因素。