Watanabe Minoru, Ishikawa Tsubasa, Kagaya Satoshi, Kuzushima Daichi, Kachi Itaru, Tanabe Satoe, Kobayashi Yasuoki, Kanzaki Koji
Department of Orthopedic Surgery, Showa University Fujigaoka Hospital, 1-30 fujigaoka Aoba-ku, Yokohama, 227-8501, Japan.
J Orthop Surg Res. 2024 Jul 31;19(1):454. doi: 10.1186/s13018-024-04951-1.
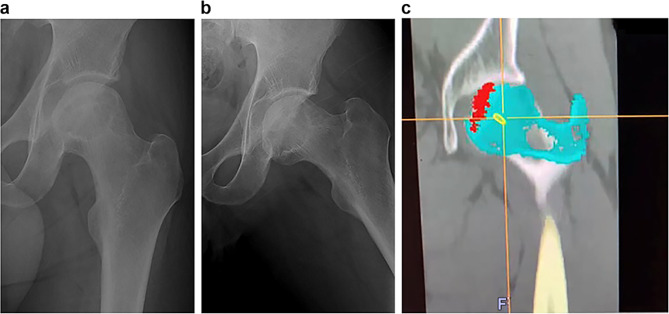
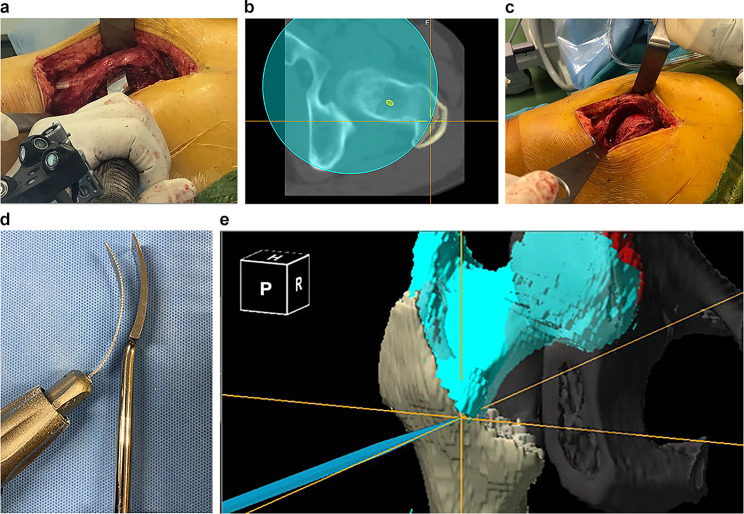
Curved varus osteotomy (CVO) is an effective femoral head-preserving surgical procedure for osteonecrosis of the femoral head (ONFH) classified as type B or C1 according to the Japanese Investigation Committee (JIC) classification; it reportedly provides better postoperative outcomes than transtrochanteric rotational osteotomy (TRO). We have developed a new procedure called spherical varus rotational osteotomy (SVRO) in which osteotomy of the femur into a spherical shape is followed by varus and anterior rotation using navigation to increase indications and improve postoperative outcomes.
Nine joints of eight patients who underwent SVRO and could be followed up for > 1 year were included in the study. Disease types determined preoperatively according to the JIC classification were type C1 for four joints and type C2 for five joints. Preoperative disease JIC classification stages were 3a for eight joints and 1 for one joint. SVRO was performed using OrthoMap 3D Navigation software, and the following variables were measured: surgery time, intraoperative blood loss, difference between preoperative and postoperative angles of anteversion, postoperative lower limb length discrepancy, and postoperative intact area occupancy. The Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ) was used for clinical evaluation. Visual Analog Scale and JHEQ scores were evaluated preoperatively and at the final follow-up.
The measurement results were as follows: surgery time, 130 min; blood loss, 200 ml; angle of varus, 20°; angle of anterior rotation, 30°; preoperative angle of anteversion, 15°; postoperative angle of anteversion, 22°; lower limb shortening, 11 mm; preoperative intact area occupancy, 0%; and postoperative intact area occupancy, 74.2%. There were no cases of progression in the postoperative stages or re-collapse.
SVRO allows for the repositioning of the exterior and posterior intact areas, providing a broader intact region postoperatively. This technique is particularly beneficial for young patients with ONFH and extensive necrosis and is a less invasive alternative to TRO. This procedure has been shown to be effective in achieving favorable outcomes in patients with extensive necrosis who would have otherwise required rotational osteotomy, depending on the necrosis location. Further longitudinal studies are necessary to validate these findings and establish long-term benefits.
根据日本调查委员会(JIC)分类,弧形内翻截骨术(CVO)是一种用于治疗股骨头坏死(ONFH)的有效保头手术,适用于B型或C1型;据报道,其术后效果优于经转子旋转截骨术(TRO)。我们开发了一种名为球形内翻旋转截骨术(SVRO)的新手术,该手术先将股骨截成球形,然后使用导航进行内翻和前旋,以扩大适应症并改善术后效果。
本研究纳入了8例接受SVRO且随访时间超过1年的患者的9个关节。术前根据JIC分类确定的疾病类型为:4个关节为C1型,5个关节为C2型。术前疾病JIC分期为:8个关节为3a期,1个关节为1期。使用OrthoMap 3D导航软件进行SVRO,并测量以下变量:手术时间、术中出血量、术前和术后前倾角的差异、术后下肢长度差异以及术后完整区域占有率。采用日本骨科协会髋关节疾病评估问卷(JHEQ)进行临床评估。术前和末次随访时评估视觉模拟量表和JHEQ评分。
测量结果如下:手术时间130分钟;出血量200毫升;内翻角度20°;前旋角度30°;术前前倾角15°;术后前倾角22°;下肢缩短11毫米;术前完整区域占有率0%;术后完整区域占有率74.2%。术后阶段无进展或再塌陷病例。
SVRO可重新定位外部和后部完整区域,术后提供更广泛的完整区域。该技术对患有ONFH且坏死范围广泛的年轻患者特别有益,是TRO的一种侵入性较小的替代方法。对于因坏死位置而异原本需要旋转截骨术的广泛坏死患者,该手术已被证明能有效取得良好效果。需要进一步的纵向研究来验证这些发现并确定长期益处。