Rivlin Katherine, Bornstein Marta, Wascher Jocelyn, Norris Turner Abigail, Norris Alison H, Howard Dana
Department of Obstetrics and Gynecology, University of Chicago Medicine, Chicago, Illinois.
Department of Health Promotion Education and Behavior, Arnold School of Public Health, University of South Carolina, Columbia.
JAMA Netw Open. 2024 Aug 1;7(8):e2426248. doi: 10.1001/jamanetworkopen.2024.26248.
Moral distress occurs when individuals feel powerless to do what they think is right, including when clinicians are prevented from providing health care they deem necessary. The loss of federal protections for abortion following the Dobbs v Jackson Women's Health Organization Supreme Court decision may place clinicians providing abortion at risk of experiencing moral distress, as many could face new legal and civil penalties for providing care in line with professional standards and that they perceive as necessary.
To assess self-reported moral distress scores among abortion-providing clinicians following the Dobbs decision overall and by state-level abortion policy.
DESIGN, SETTING, AND PARTICIPANTS: This survey study, conducted from May to December 2023, included US abortion-providing clinicians (physicians, advanced practice clinicians, and nurses). A purposive electronic survey was disseminated nationally through professional listservs and snowball sampling.
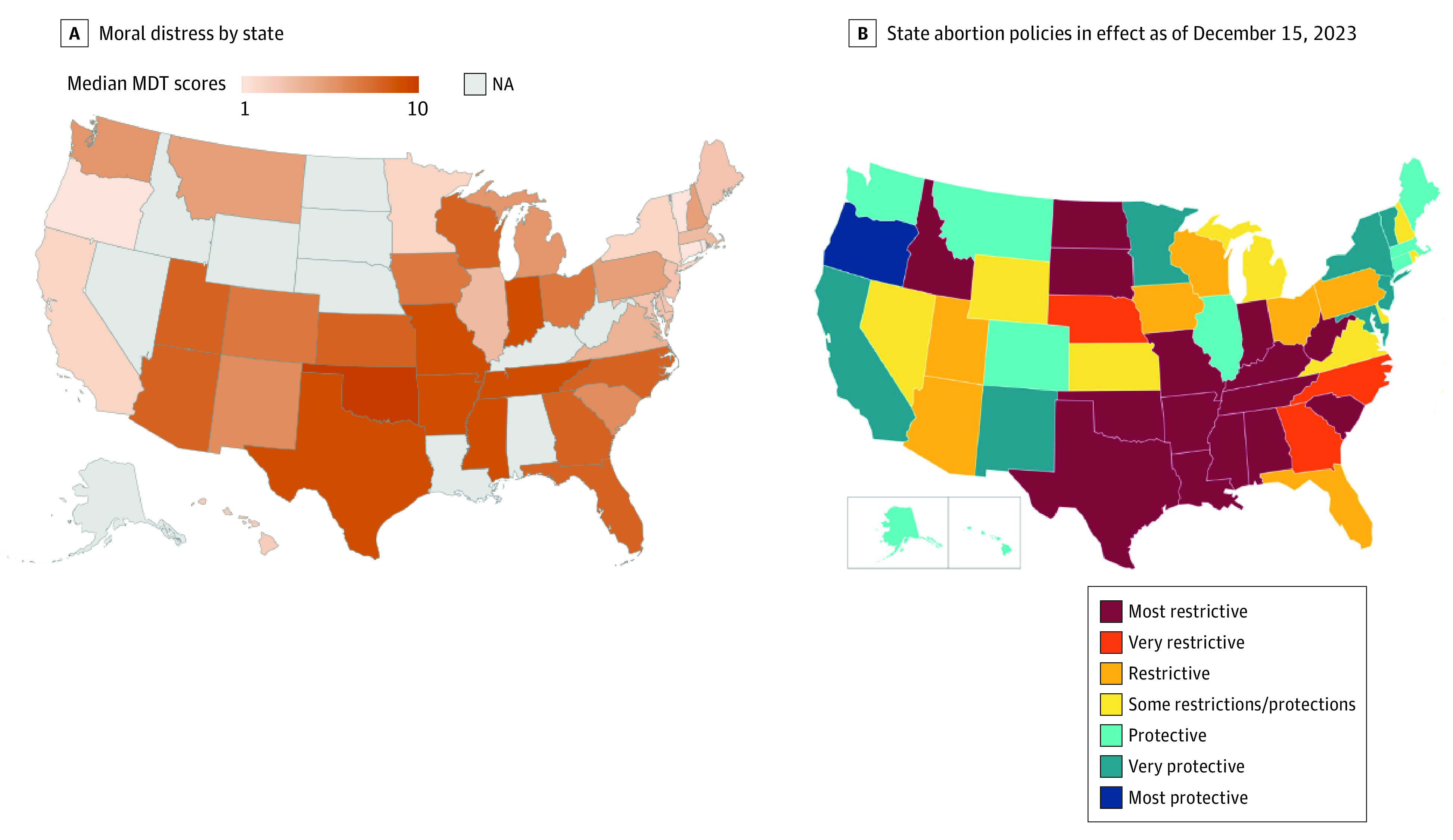
Abortion policy in each respondent's state of practice (restrictive vs protective using classifications from the Guttmacher Institute).
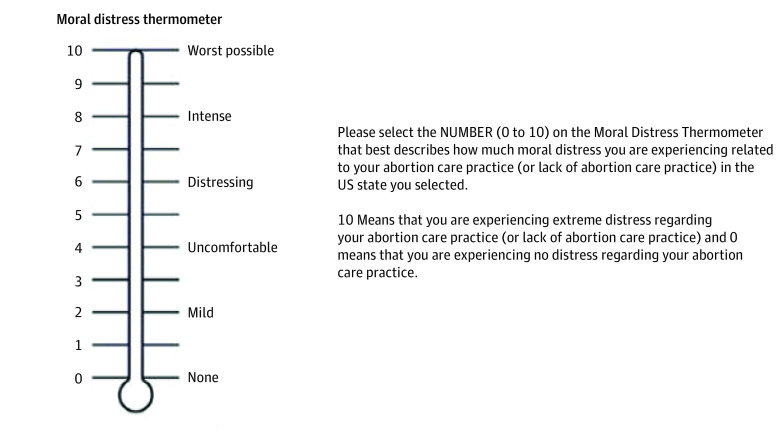
Using descriptive statistics and unadjusted and adjusted negative binomial regression models, the association between self-reported moral distress on the Moral Distress Thermometer (MDT), a validated psychometric tool that scores moral distress from 0 (none) to 10 (worst possible), and state abortion policy was examined.
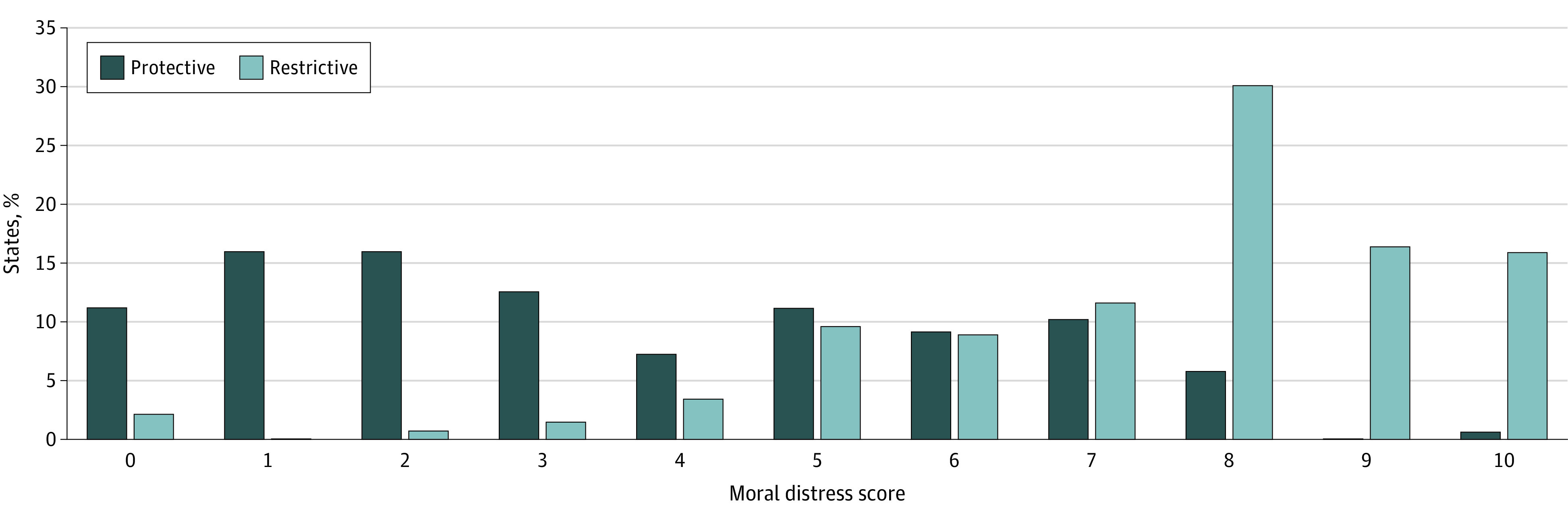
Overall, 310 clinicians (271 [87.7%] women; mean [SD] age, 41.4 [9.7] years) completed 352 MDTs, with 206 responses (58.5%) from protective states and 146 (41.5%) from restrictive states. Reported moral distress scores ranged from 0 to 10 (median, 5) and were more than double for clinicians in restrictive compared with protective states (median, 8 [IQR, 6-9] vs 3 [IQR, 1-6]; P < .001). Respondents with higher moral distress scores included physicians compared with advanced practice clinicians (median, 6 [IQR, 3-8] vs 4 [IQR, 2-7]; P = .005), those practicing in free-standing abortion clinics compared with those practicing in hospitals (median, 6 [IQR, 3-8] vs 4 [IQR, 2-7]; P < .001), those no longer providing abortion care compared with those still providing abortion care (median, 8 [IQR, 4-9] vs 5 [IQR, 2-8]; P = .004), those practicing in loss states (states with the greatest decline in abortion volume since the Dobbs decision) compared with those in stable states (unadjusted incidence rate [IRR], 1.72 [95% CI, 1.55-1.92]; P < .001; adjusted IRR, 1.59 [95% CI, 1.40-1.79]; P < .001), and those practicing in surge states (states with the greatest increase in abortion volume since the Dobbs decision) compared with those in stable states (unadjusted IRR, 1.27 [95% CI, 1.11-1.46]; P < .001; adjusted IRR, 1.24 [95% CI, 1.09-1.41]; P = .001).
In this purposive national survey study of clinicians providing abortion, moral distress was elevated among all clinicians and more than twice as high among those practicing in states that restrict abortion compared with those in states that protect abortion. The findings suggest that structural changes addressing bans on necessary health care, such as federal protections for abortion, are needed at institutional, state, and federal policy levels to combat widespread moral distress.
当个人感到无力去做他们认为正确的事情时,就会出现道德困扰,包括临床医生被阻止提供他们认为必要的医疗保健服务时。在多布斯诉杰克逊妇女健康组织最高法院裁决之后,联邦对堕胎的保护措施丧失,这可能使提供堕胎服务的临床医生面临道德困扰的风险,因为许多人可能因按照专业标准提供他们认为必要的护理而面临新的法律和民事处罚。
评估多布斯裁决后,提供堕胎服务的临床医生总体上以及按州级堕胎政策划分的自我报告的道德困扰得分。
设计、背景和参与者:这项调查研究于2023年5月至12月进行,纳入了美国提供堕胎服务的临床医生(医生、高级执业临床医生和护士)。通过专业邮件列表和滚雪球抽样在全国范围内开展了一项有目的的电子调查。
每个受访者执业所在州的堕胎政策(使用古特马赫研究所的分类,分为限制性政策与保护性政策)。
使用描述性统计以及未调整和调整后的负二项回归模型,研究了在道德困扰温度计(MDT)上自我报告的道德困扰之间的关联,MDT是一种经过验证的心理测量工具,对道德困扰的评分从0(无)到10(可能的最严重程度),并研究了州堕胎政策。
总体而言,310名临床医生(271名[87.7%]为女性;平均[标准差]年龄为41.4[9.7]岁)完成了352份MDT问卷,其中来自保护性州的有206份回复(58.5%),来自限制性州的有146份(41.5%)。报告的道德困扰得分范围为0至10(中位数为5),与保护性州的临床医生相比,限制性州的临床医生的得分高出一倍多(中位数,8[四分位间距,6 - 9]对3[四分位间距,1 - 6];P <.001)。道德困扰得分较高的受访者包括医生,与高级执业临床医生相比(中位数,6[四分位间距,3 - 8]对4[四分位间距,2 - 7];P = 0.005),在独立堕胎诊所执业的医生与在医院执业的医生相比(中位数,6[四分位间距,3 - 8]对4[四分位间距,2 - 7];P <.001),不再提供堕胎护理的医生与仍在提供堕胎护理的医生相比(中位数,8[四分位间距,4 - 9]对5[四分位间距,2 - 8];P = 0.004),在堕胎量减少的州(自多布斯裁决以来堕胎量下降最大的州)执业的医生与在稳定州执业的医生相比(未调整发病率比[IRR],1.72[95%置信区间,1.55 - 1.92];P <.001;调整后IRR,1.59[95%置信区间,1.40 - 1.79];P <.001),以及在堕胎量激增的州(自多布斯裁决以来堕胎量增加最大的州)执业的医生与在稳定州执业的医生相比(未调整IRR,1.27[95%置信区间,1.11 - 1.46];P <.001;调整后IRR,1.24[95%置信区间,1.09 - 1.41];P = 0.001)。
在这项针对提供堕胎服务的临床医生的有目的的全国性调查研究中,所有临床医生的道德困扰都有所加剧,与那些在保护堕胎的州执业的医生相比,在限制堕胎的州执业的医生的道德困扰高出两倍多。研究结果表明,在机构、州和联邦政策层面,需要进行结构性变革以应对对必要医疗保健的禁令,例如对堕胎的联邦保护,以对抗广泛存在的道德困扰。