Ophthalmology Clinic Vista Sánchez Trancón, Vista Sánchez Trancón Building Tecnolaser, Room 14 Calle La Violeta, Badajoz, 06005, Spain.
Centre of Physics, University of Minho, Braga, Portugal.
BMC Ophthalmol. 2024 Aug 1;24(1):321. doi: 10.1186/s12886-024-03529-z.
Assessing refractive errors under cycloplegia is recommended for paediatric patients; however, this may not always be feasible. In these situations, refraction has to rely on measurements made under active accommodation which may increase measurements variability and error. Therefore, evaluating the accuracy and precision of non-cycloplegic refraction and biometric measurements is clinically relevant. The Myopia Master, a novel instrument combining autorefraction and biometry, is designed for monitoring refractive error and ocular biometry in myopia management. This study assessed its repeatability and agreement for autorefraction and biometric measurements pre- and post-cycloplegia.
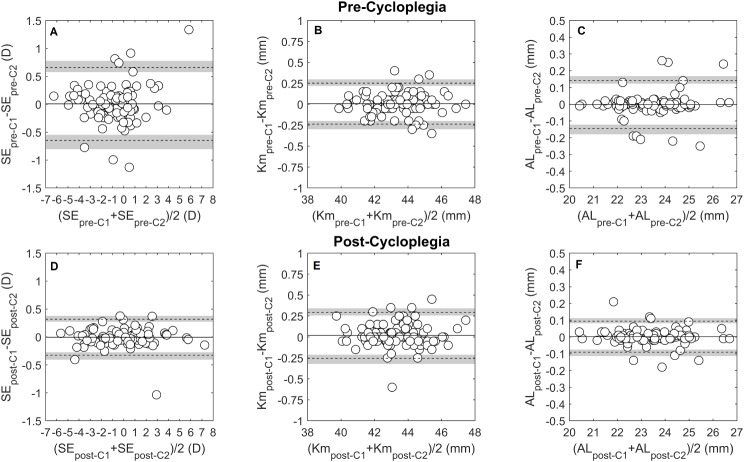
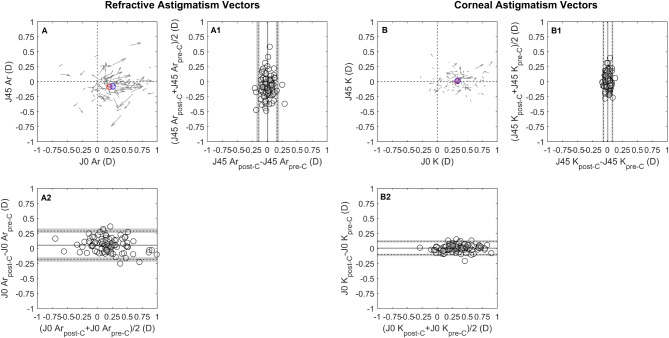
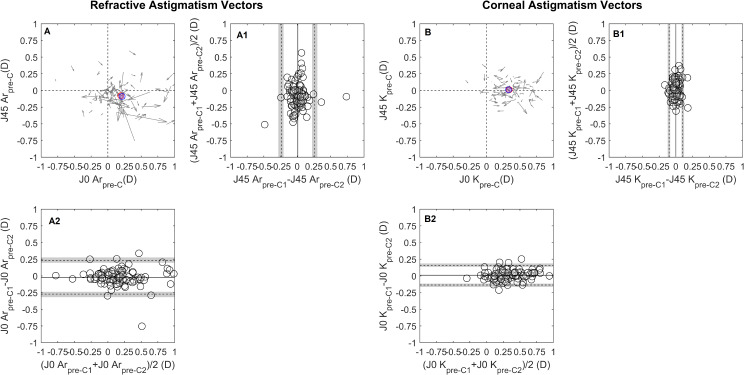
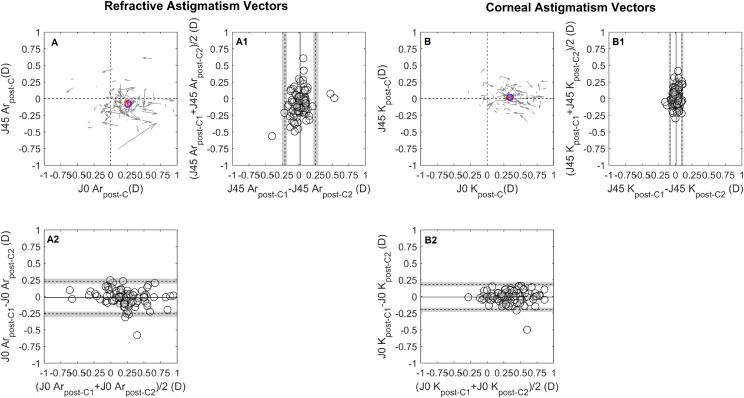
A prospective cross-sectional study evaluated a cohort of 96 paediatric patients that underwent ophthalmologic examination. An optometrist performed two repeated measurements of autorefraction and biometry pre- and post-cycloplegia. Test-retest repeatability (TRT) was assessed as differences between consecutive measurements and agreement as differences between post- and pre-cycloplegia measurements, for spherical equivalent (SE), refractive and keratometric J0/J45 astigmatic components, mean keratometry (Km) and axial length (AL).
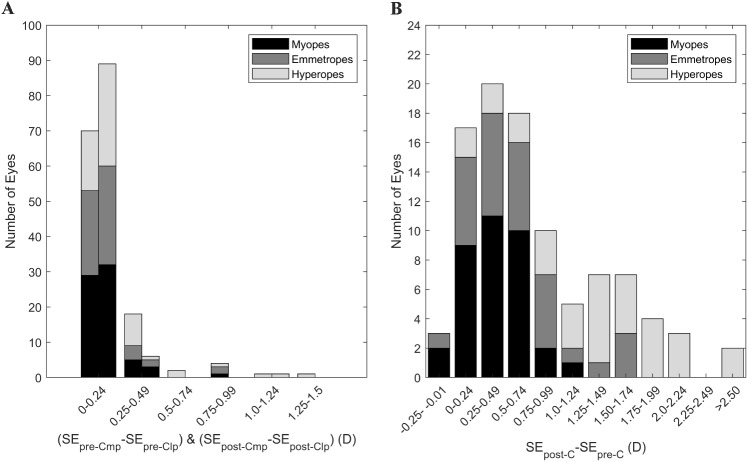
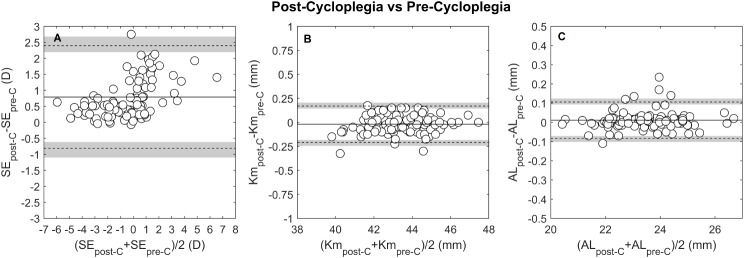
Cycloplegia significantly improved the SE repeatability (TRT, pre-cyclo: 0.65 D, post-cyclo: 0.31 D). SE measurements were more repeatable in myopes and emmetropes compared to hyperopes. Keratometry (Km) repeatability did not change with cycloplegia (TRT, pre-cyclo: 0.25 D, post-cyclo:0.27 D) and AL repeatability improved marginally (TRT, pre-cyclo: 0.14 mm, post-cyclo: 0.09 mm). Regarding pre- and post-cycloplegia agreement, SE became more positive by + 0.79 D, varying with refractive error. Myopic eyes showed a mean difference of + 0.31 D, while hyperopes differed by + 1.57 D. Mean keratometry, refractive and keratometric J0/J45 and AL showed no clinically significant differences.
Refractive error measurements, using the Myopia Master were 2.5x less precise pre-cycloplegia than post-cycloplegia. Accuracy of pre-cycloplegic refractive error measurements was often larger than the clinically significant threshold (0.25 D) and was refractive error dependent. The higher precision compared to autorefraction measurements, pre- and post-cycloplegia agreement and refractive error independence of AL measurements emphasize the superiority of AL in refractive error monitoring.
在睫状肌麻痹下评估屈光不正,这是推荐用于儿科患者的;然而,这并不总是可行的。在这些情况下,折射必须依靠主动调节下的测量,这可能会增加测量的可变性和误差。因此,评估非睫状肌麻痹下的折射和生物测量的准确性和精密度在临床上是相关的。Myopia Master 是一种结合自动折射和生物测量的新型仪器,用于监测近视管理中的屈光误差和眼生物测量。本研究评估了其在睫状肌麻痹前后的自动折射和生物测量的重复性和一致性。
前瞻性横断面研究评估了 96 名接受眼科检查的儿科患者队列。一名验光师对睫状肌麻痹前后进行了两次自动折射和生物测量的重复测量。测试-再测试重复性(TRT)作为连续测量之间的差异进行评估,而一致性则作为睫状肌麻痹前后测量之间的差异进行评估,用于评估球镜等效(SE)、折射和角膜 J0/J45 散光分量、平均角膜曲率(Km)和眼轴(AL)。
睫状肌麻痹显著改善了 SE 的重复性(TRT,预环:0.65D,后环:0.31D)。与远视相比,近视和正视者的 SE 测量更具重复性。角膜曲率(Km)重复性不因睫状肌麻痹而改变(TRT,预环:0.25D,后环:0.27D),眼轴(AL)重复性略有改善(TRT,预环:0.14mm,后环:0.09mm)。关于睫状肌麻痹前后的一致性,SE 变为正的 +0.79D,与屈光不正有关。近视眼的平均差值为+0.31D,而远视眼的差值为+1.57D。平均角膜曲率、折射和角膜 J0/J45 以及 AL 无临床显著差异。
使用 Myopia Master 进行屈光不正测量,在睫状肌麻痹前比睫状肌麻痹后精度低 2.5 倍。睫状肌麻痹前屈光不正测量的准确性通常大于临床显著阈值(0.25D),并且与屈光不正有关。与自动折射测量相比,更高的精度,在睫状肌麻痹前后的一致性和 AL 测量的屈光不正独立性,强调了 AL 在屈光不正监测中的优越性。