Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Lancet Healthy Longev. 2024 Aug;5(8):e563-e573. doi: 10.1016/S2666-7568(24)00131-4. Epub 2024 Jul 30.
Deprescribing of antihypertensive medications is recommended for some older patients with low blood pressure and frailty. The OPTiMISE trial showed that this deprescribing can be achieved with no differences in blood pressure control at 3 months compared with usual care. We aimed to examine effects of deprescribing on longer-term hospitalisation and mortality.
This randomised controlled trial enrolled participants from 69 general practices across central and southern England. Participants aged 80 years or older, with systolic blood pressure less than 150 mm Hg and who were receiving two or more antihypertensive medications, were randomly assigned (1:1) to antihypertensive medication reduction (removal of one antihypertensive) or usual care. General practitioners and participants were aware of the treatment allocation following randomisation but individuals responsible for analysing the data were masked to the treatment allocation throughout the study. Participants were followed up via their primary and secondary care electronic health records at least 3 years after randomisation. The primary outcome was time to all-cause hospitalisation or mortality. Intention-to-treat analyses were done using Cox regression modelling. A per-protocol analysis of the primary outcome was also done, excluding participants from the intervention group who did not reduce treatment or who had medication reinstated during the initial trial 12-week follow-up period. This study is registered with the European Union Drug Regulating Authorities Clinical Trials Database (EudraCT2016-004236-38) and the ISRCTN Registry (ISRCTN97503221).
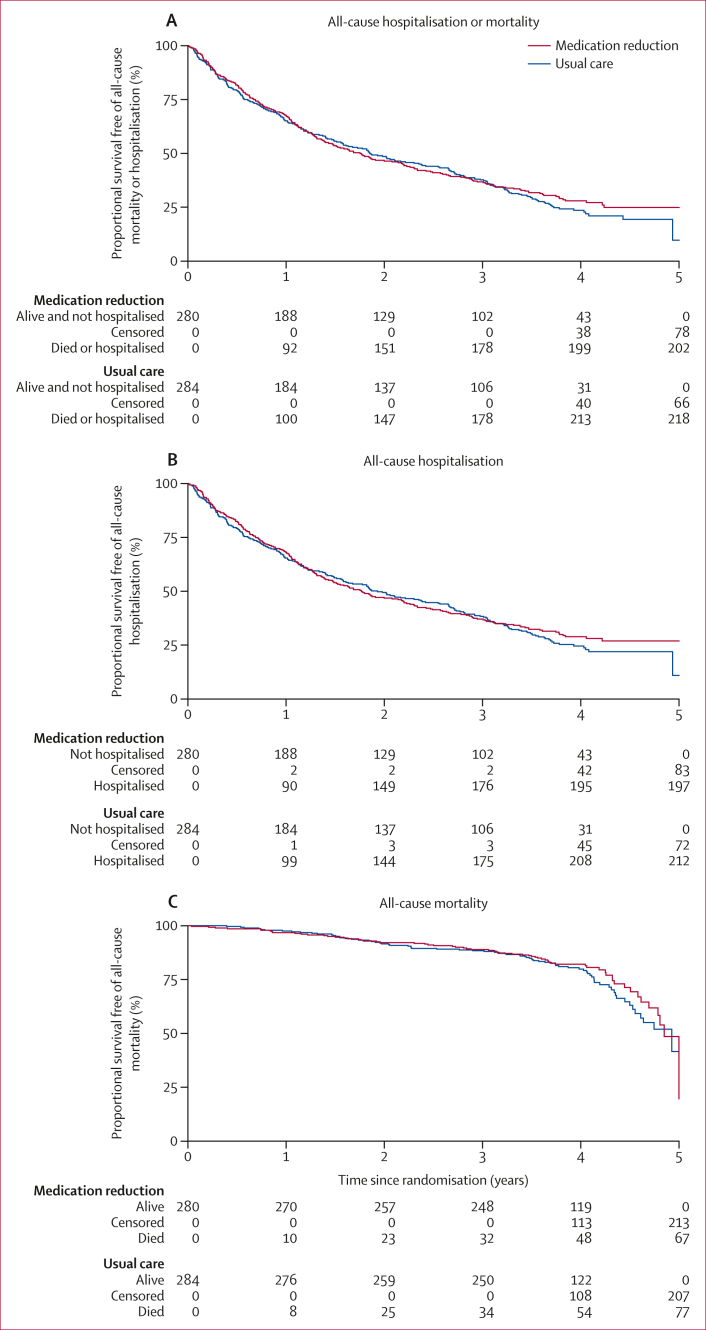
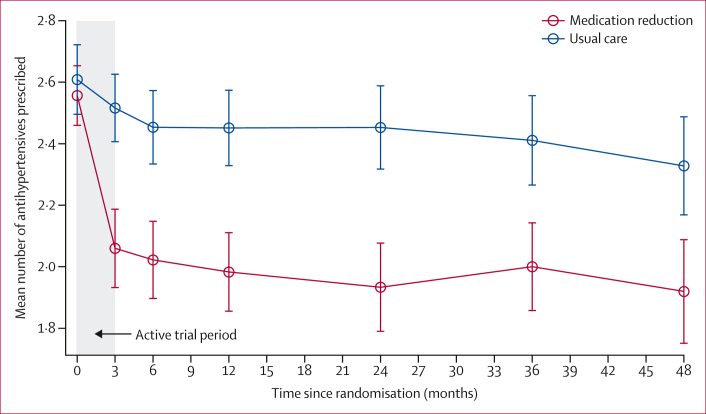
Between March 20, 2017, and Sept 30, 2018, a total of 569 participants were randomly assigned. Of these, 564 (99%; intervention=280; control=284) were followed up for a median of 4·0 years (IQR 3·7-4·3). Participants had a mean age of 84·8 years (SD 3·4) at baseline and 273 (48%) were women. Medication reduction was sustained in 109 participants at follow-up (51% of the 213 participants alive in the intervention group). Participants in the intervention group had a larger reduction in antihypertensives than the control group (adjusted mean difference -0·35 drugs [95% CI -0·52 to -0·18]). Overall, 202 (72%) participants in the intervention group and 218 (77%) participants in the control group experienced hospitalisation or mortality during follow-up (adjusted hazard ratio [aHR] 0·93 [95% CI 0·76 to 1·12]). There was some evidence that the proportion of participants experiencing the primary outcome in the per-protocol population was lower in the intervention group (aHR 0·80 [0·64 to 1·00]).
Half of participants sustained medication reduction with no evidence of an increase in all-cause hospitalisation or mortality. These findings suggest that an antihypertensive deprescribing intervention might be safe for people aged 80 years or older with controlled blood pressure taking two or more antihypertensives.
British Heart Foundation and National Institute for Health and Care Research.
对于一些血压较低且虚弱的老年患者,建议减少降压药物的使用。OPTiMISE 试验表明,与常规护理相比,在 3 个月时,这种药物减少不会导致血压控制出现差异。我们旨在研究药物减少对长期住院和死亡率的影响。
这项随机对照试验招募了来自英格兰中部和南部 69 家普通诊所的参与者。年龄在 80 岁及以上、收缩压低于 150mmHg 且正在服用两种或更多种降压药物的患者被随机分配(1:1)接受降压药物减少(一种降压药物的去除)或常规护理。在随机分组后,全科医生和参与者都知道治疗分配情况,但负责分析数据的人员在整个研究过程中对治疗分配情况一无所知。通过他们的初级和二级医疗电子健康记录对参与者进行了至少 3 年的随访。主要结局是全因住院或死亡的时间。使用 Cox 回归模型进行意向治疗分析。还对主要结局进行了符合方案分析,排除了干预组中未减少治疗或在初始试验的 12 周随访期间重新开始用药的参与者。本研究在欧盟药品监管当局临床试验数据库(EudraCT2016-004236-38)和 ISRCTN 登记处(ISRCTN97503221)注册。
2017 年 3 月 20 日至 2018 年 9 月 30 日,共有 569 名参与者被随机分配。其中,564 名(99%;干预组 280 名;对照组 284 名)在中位随访 4.0 年(IQR 3.7-4.3)后进行了随访。参与者的基线平均年龄为 84.8 岁(SD 3.4),273 名(48%)为女性。在随访时,有 109 名参与者(干预组中存活的 213 名参与者中的 51%)维持了药物减少。与对照组相比,干预组的降压药物减少幅度更大(调整后的平均差异-0.35 种药物[95%CI-0.52 至-0.18])。在随访期间,干预组有 202 名(72%)参与者和对照组有 218 名(77%)参与者经历了住院或死亡(调整后的危险比[aHR]0.93[95%CI0.76 至 1.12])。有一些证据表明,在符合方案的人群中,干预组中经历主要结局的参与者比例较低(aHR 0.80[0.64 至 1.00])。
一半的参与者维持了药物减少,且全因住院或死亡率没有增加。这些发现表明,对于血压控制良好且服用两种或更多种降压药物的 80 岁及以上的患者,进行降压药物减少干预可能是安全的。
英国心脏基金会和国家卫生与保健研究所。