Hörmandinger Christina, Bitschi David, Berthold Daniel P, Neidlein Claas, Schroeder Lennart, Watrinet Julius, Pätzold Robert, Böcker Wolfgang, Holzapfel Boris Michael, Fürmetz Julian, Bormann Markus
Department of Orthopaedics and Trauma Surgery, Musculoskeletal University Center Munich (MUM), University Hospital, LMU Munich, Marchioninistraße 15, 81377, Munich, Germany.
Department of Trauma Surgery, Trauma Center Murnau, Murnau am Staffelsee, Germany.
Eur J Trauma Emerg Surg. 2024 Dec;50(6):2937-2945. doi: 10.1007/s00068-024-02616-6. Epub 2024 Aug 2.
In recent years, the trauma mechanisms and fracture types in tibial plateau fractures (TPF) have changed. At the same time, treatment strategies have expanded with the establishment of new classification systems, extension of diagnostics and surgical strategies. Evidence-based recommendations for treatment strategies are rare. The aim of this study is to assess the extent of standardization in the treatment of complex TPF.
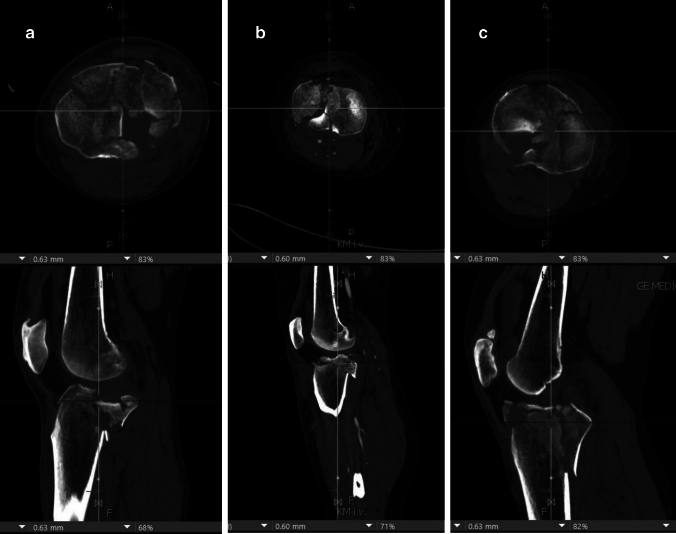
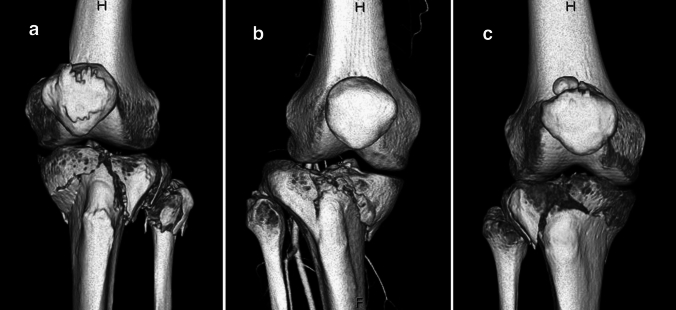
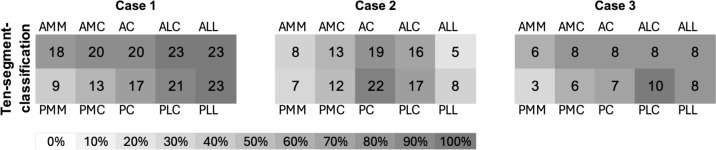
For the study, specialists in trauma surgery/orthopaedics were presented thin-slice CT data sets of three complex TPFs including 3D reconstructions. A standardized questionnaire on fracture morphology and planned treatment strategy was then completed.
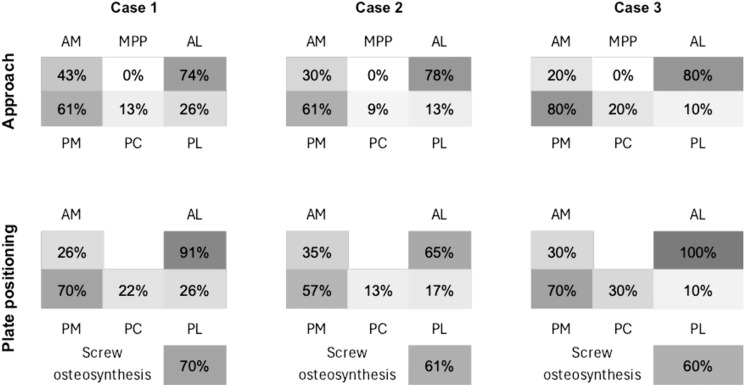
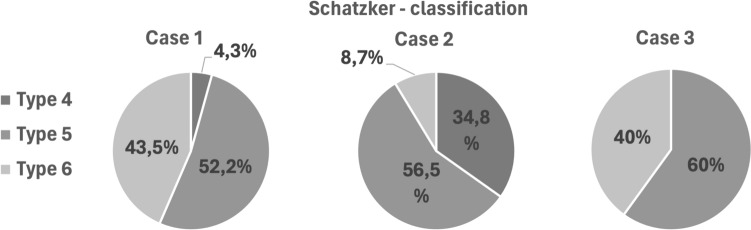
A total of 23 surgeons from 7 hospitals (Trauma center levels I-III) were included. All three fractures were most frequently classified as Schatzker type V (fracture I: 52.2%, II: 56.5%, III: 60%). Averaged over all three fractures, 55% of the respondents chose the same patient positioning. The combination of a posteromedial and anterolateral approach was the most frequently chosen approach at 42.7%. Double plating was favored for the surgical treatment of all fractures (70.7%). Preoperative MRI, extended approaches and intraoperative fraturoscopy were significantly more common in level I trauma centres.
There are major differences in the management of complex TPF. 360° treatment is carried out in all departments regardless of the level of care, but without further standardization in terms of preoperative imaging, classification, initial treatment, approach, fixation and intraoperative imaging. There are major differences within the departments with different level of care.
近年来,胫骨平台骨折(TPF)的创伤机制和骨折类型发生了变化。与此同时,随着新分类系统的建立、诊断和手术策略的扩展,治疗策略也有所增加。关于治疗策略的循证推荐很少。本研究的目的是评估复杂TPF治疗的标准化程度。
在本研究中,向创伤外科/骨科专家展示了三个复杂TPF的薄层CT数据集,包括三维重建。然后完成一份关于骨折形态和计划治疗策略的标准化问卷。
共纳入了来自7家医院(一级至三级创伤中心)的23名外科医生。所有三处骨折最常被分类为Schatzker V型(骨折I:52.2%,II:56.5%,III:60%)。在所有三处骨折中,平均55%的受访者选择了相同的患者体位。后内侧和前外侧联合入路是最常选择的入路,占42.7%。所有骨折的手术治疗均倾向于双钢板固定(70.7%)。术前MRI、扩大入路和术中关节镜检查在一级创伤中心更为常见。
复杂TPF的治疗存在重大差异。所有科室无论护理级别如何都采用360°治疗,但在术前影像学、分类、初始治疗、入路、固定和术中影像学方面没有进一步的标准化。不同护理级别的科室之间存在重大差异。