Temerty Faculty of Medicine, University of Toronto, Toronto, Canada.
Humber River Health, Toronto, Canada.
BMC Health Serv Res. 2024 Aug 5;24(1):893. doi: 10.1186/s12913-024-11281-9.
Federal deregulation of opioid agonist therapies are an attractive policy option to improve access to opioid use disorder care and achieve widespread beneficial impacts on growing opioid-related harms. There have been few evaluations of such policy interventions and understanding effects can help policy planning across jurisdictions.
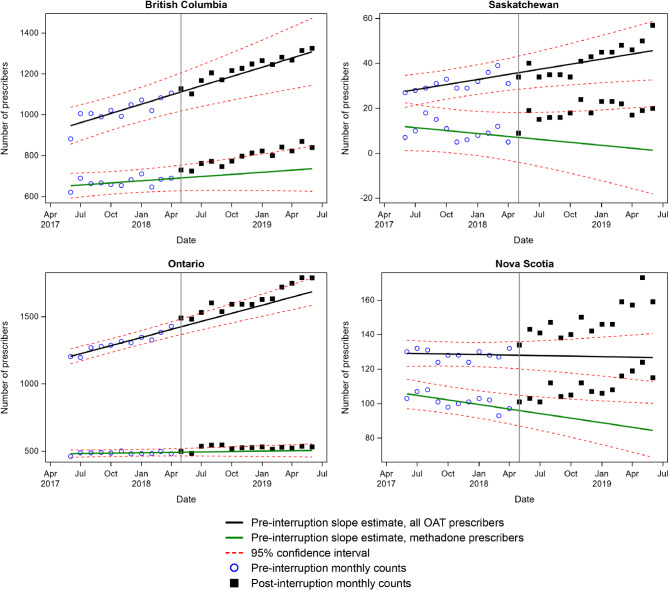
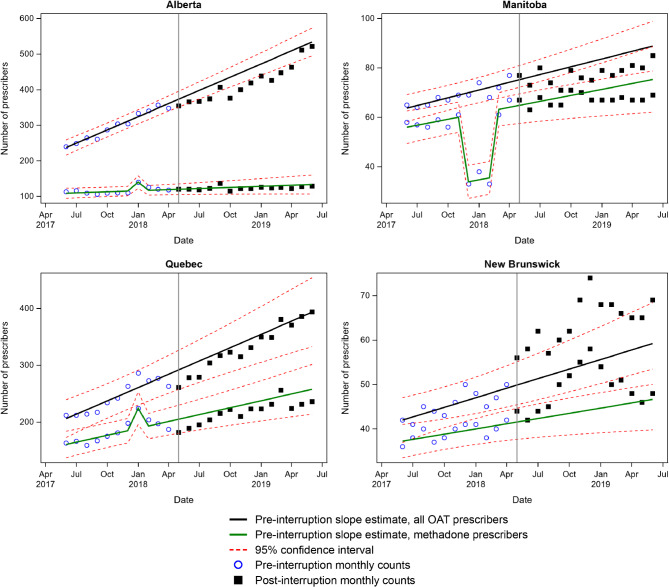
Using health administrative data from eight of ten Canadian provinces, this study evaluated the impacts of Health Canada's decision in May 2018 to rescind the requirement for Canadian health professionals to obtain an exemption from the Canadian Drugs and Substance Act to prescribe methadone for opioid use disorder. Over the study period of June 2017 to May 2019, we used descriptive statistics to capture overall trends in the number of agonist therapy prescribers across provinces and we used interrupted time series analysis to determine the effect of this decision on the trajectories of the agonist therapy prescribing workforces.
There were important baseline differences in the numbers of agonist therapy prescribers. The province with the highest concentration of prescribers had 7.5 more prescribers per 100,000 residents compared to the province with the lowest. All provinces showed encouraging growth in the number of prescribers through the study period, though the fastest growing province grew 4.5 times more than the slowest. Interrupted time series analyses demonstrated a range of effects of the federal policy intervention on the provinces, from clearly positive changes to possibly negative effects.
Federal drug regulation policy change interacted in complex ways with provincial health professional regulation and healthcare delivery, kaleidoscoping the effects of federal policy intervention. For Canada and other health systems such as the US, federal policy must account for significant subnational variation in OUD epidemiology and drug regulation to maximize intended beneficial effects and mitigate the risks of negative effects.
放宽阿片类激动剂疗法的联邦监管是改善获得阿片类药物使用障碍治疗的机会并实现广泛的有益影响以应对日益严重的阿片类相关危害的一个有吸引力的政策选择。对于这种政策干预措施,评估的研究很少,了解其效果有助于各司法管辖区的政策规划。
本研究使用来自加拿大十个省份中的八个省份的卫生行政数据,评估了加拿大卫生部 2018 年 5 月决定取消加拿大卫生专业人员必须获得《加拿大毒品和药物法》豁免才能开处美沙酮治疗阿片类药物使用障碍的要求的政策干预的影响。在 2017 年 6 月至 2019 年 5 月的研究期间,我们使用描述性统计来捕捉全省阿片激动剂治疗师数量的总体趋势,并使用中断时间序列分析来确定这一决定对阿片激动剂治疗师队伍发展轨迹的影响。
阿片类激动剂治疗师的数量存在重要的基线差异。有较多治疗师的省份每 10 万居民中有 7.5 名治疗师,而最少的省份则有 7.5 名治疗师。所有省份在研究期间都显示出治疗师人数的可喜增长,尽管增长最快的省份比增长最慢的省份增长了 4.5 倍。中断时间序列分析表明,联邦政策干预对各省份的影响范围广泛,从明显的积极变化到可能的负面影响。
联邦药物管制政策的变化以复杂的方式与省级卫生专业人员的监管和医疗保健提供相互作用,使联邦政策干预的效果变得多样化。对于加拿大和美国等其他卫生系统,联邦政策必须考虑到阿片类药物使用障碍的流行病学和药物管制方面的重大国家差异,以最大限度地发挥预期的有益效果并减轻不利影响的风险。