School of Public Health, The University of Queensland, Brisbane, Australia.
College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia.
BMC Health Serv Res. 2024 Aug 5;24(1):895. doi: 10.1186/s12913-024-11351-y.
Patients with multiple long-term conditions requires understanding the existing care models to address their complex and multifaceted health needs. However, current literature lacks a comprehensive overview of the essential components, impacts, challenges, and facilitators of these care models, prompting this scoping review.
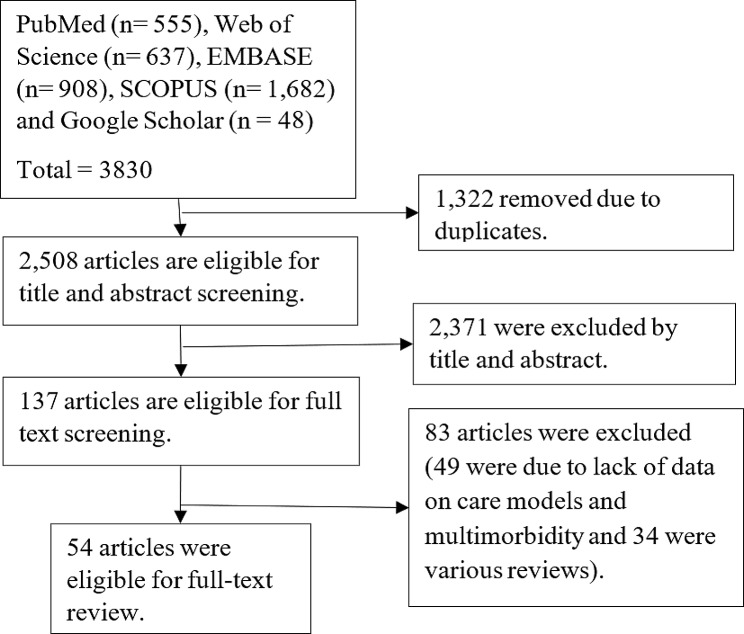
A scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis Extension for Scoping Reviews guideline. Our search encompassed articles from PubMed, Web of Science, EMBASE, SCOPUS, and Google Scholar. The World Health Organization's health system framework was utilized to synthesis the findings. This framework comprises six building blocks (service delivery, health workforce, health information systems, access to essential medicines, financing, and leadership/governance) and eight key characteristics of good service delivery models (access, coverage, quality, safety, improved health, responsiveness, social and financial risk protection, and improved efficiency). Findings were synthesized qualitatively to identify components, impacts, barriers, and facilitators of care models.
A care model represents various collective interventions in the healthcare delivery aimed at achieving desired outcomes. The names of these care models are derived from core activities or major responsibilities, involved healthcare teams, diseases conditions, eligible clients, purposes, and care settings. Notable care models include the Integrated, Collaborative, Integrated-Collaborative, Guided, Nurse-led, Geriatric, and Chronic care models, as well as All-inclusive Care Model for the Elderly, IMPACT clinic, and Geriatric Patient-Aligned Care Teams (GeriPACT). Other care models (include Care Management Plus, Value Stream Mapping, Preventive Home Visits, Transition Care, Self-Management, and Care Coordination) have supplemented the main ones. Care models improved quality of care (such as access, patient-centeredness, timeliness, safety, efficiency), cost of care, and quality of life for patients that were facilitated by presence of shared mission, system and function integration, availability of resources, and supportive tools.
Care models were implemented for the purpose of enhancing quality of care, health outcomes, cost efficiency, and patient satisfaction by considering careful recruitment of eligible clients, appropriate selection of service delivery settings, and robust organizational arrangements involving leadership roles, healthcare teams, financial support, and health information systems. The distinct team compositions and their roles in service provision processes differentiate care models.
患有多种长期疾病的患者需要了解现有的护理模式,以满足他们复杂和多方面的健康需求。然而,目前的文献缺乏对这些护理模式的基本组成部分、影响、挑战和促进因素的全面概述,因此需要进行这一范围界定综述。
根据系统评价和荟萃分析扩展的首选报告项目用于范围界定综述的指南进行了范围界定综述。我们的搜索涵盖了来自 PubMed、Web of Science、EMBASE、SCOPUS 和 Google Scholar 的文章。利用世界卫生组织的卫生系统框架来综合研究结果。该框架包括六个组成部分(服务提供、卫生人力、卫生信息系统、基本药物获取、筹资和领导力/治理)和良好服务提供模式的八个关键特征(可及性、覆盖范围、质量、安全性、改善健康、响应性、社会和财务风险保护以及提高效率)。通过定性综合研究结果,确定了护理模式的组成部分、影响、障碍和促进因素。
护理模式代表了医疗保健提供中旨在实现预期结果的各种集体干预措施。这些护理模式的名称源自核心活动或主要职责、涉及的医疗保健团队、疾病状况、合格客户、目的和护理环境。值得注意的护理模式包括综合型、协作型、综合协作型、指导型、护士主导型、老年型和慢性护理模式,以及老年综合护理模式、IMPACT 诊所和老年患者协调护理团队(GeriPACT)。其他护理模式(包括护理管理加、流程映射、预防性家访、过渡护理、自我管理和护理协调)补充了主要模式。护理模式通过共同使命的存在、系统和功能的整合、资源的可用性以及支持性工具,改善了患者的护理质量(如可及性、以患者为中心、及时性、安全性、效率)、护理成本和生活质量。
护理模式的实施旨在通过仔细招募合格的客户、适当选择服务提供环境以及涉及领导力角色、医疗保健团队、财务支持和卫生信息系统的强大组织安排来提高护理质量、健康结果、成本效益和患者满意度。护理模式的区别在于其独特的团队组成及其在服务提供过程中的角色。