Yamada Keita, Ida-Ichikawa Mizuki, Fujimoto Naoki, Ishida Masaki, Dohi Kaoru
Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu, Mie 5148507, Japan.
Department of Radiology, Mie University Graduate School of Medicine, Tsu, Mie, Japan.
Eur Heart J Case Rep. 2024 Jul 23;8(8):ytae355. doi: 10.1093/ehjcr/ytae355. eCollection 2024 Aug.
Takotsubo syndrome (TTS) is characterized by transient regional left ventricular (LV) dysfunction occurring in individuals exposed to physical or emotional stress. Various stressors are triggers for TTS in cancer patients, and anti-cancer drugs have recently been proposed as a trigger. Therefore, further studies are needed to clarify these triggers and avoid the unnecessary interruption of anti-cancer treatment.
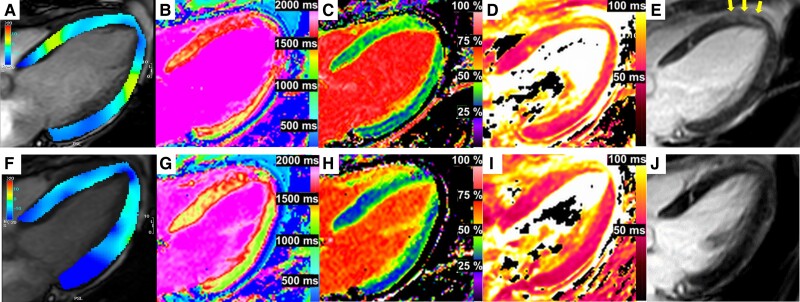
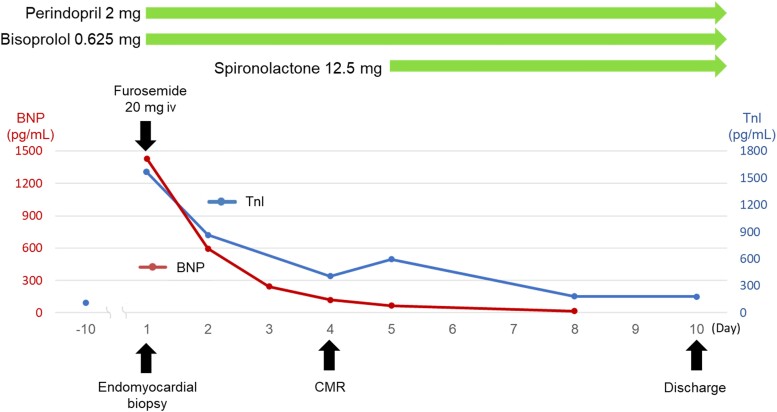
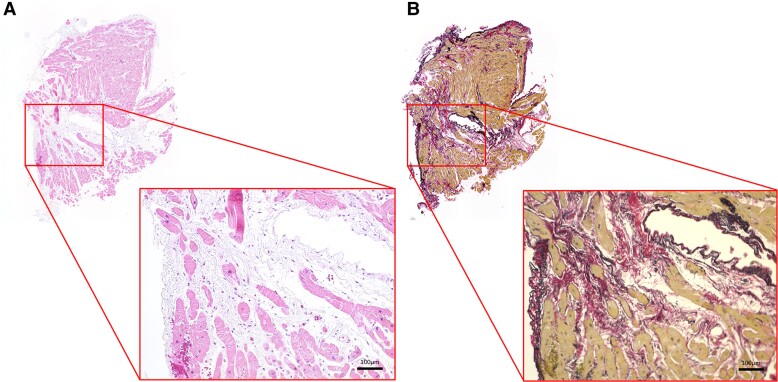
A 66-year-old woman presented with dyspnoea 10 days after the initiation of atezolizumab in combination with bevacizumab. She had previously received osimertinib as first-line therapy for recurrent lung cancer after primary resection and atezolizumab in combination with bevacizumab, paclitaxel, and carboplatin as second-line therapy. She was admitted due to electrocardiography abnormalities and elevated troponin I and brain natriuretic peptide levels. Echocardiography revealed circumferential severe LV hypokinesis at the mid-ventricular level, with preserved wall motion at the base and apex. Cardiac catheterization performed after the attenuation of symptoms with 20 mg of intravenous furosemide showed normal coronary arteries. Cardiac magnetic resonance imaging on Day 4 revealed increases in T and T values and extracellular volume fraction; however, neither myocardial infiltration of inflammatory cells or myocardial necrosis was observed in endomyocardial samples obtained on the day of her arrival. Atypical TTS was suspected, and she was treated with perindopril, bisoprolol, and spironolactone. Magnetic resonance imaging 1.5 months after the onset of TTS showed improvements in LV contractility, T and T values, and the extracellular volume fraction.
A more detailed understanding of the relationship between anti-cancer drugs and TTS is crucial for preventing interruptions to anti-cancer therapy.
应激性心肌病(TTS)的特征是在经历身体或情绪应激的个体中出现短暂的局部左心室(LV)功能障碍。各种应激源是癌症患者发生TTS的触发因素,最近有研究提出抗癌药物也是一种触发因素。因此,需要进一步研究以明确这些触发因素,并避免不必要地中断抗癌治疗。
一名66岁女性在开始使用阿替利珠单抗联合贝伐单抗治疗10天后出现呼吸困难。她之前曾接受奥希替尼作为原发性切除术后复发性肺癌的一线治疗,以及阿替利珠单抗联合贝伐单抗、紫杉醇和卡铂作为二线治疗。她因心电图异常以及肌钙蛋白I和脑钠肽水平升高而入院。超声心动图显示心室中部水平出现环形严重左心室运动减弱,而心底和心尖部壁运动保留。在静脉注射20 mg呋塞米症状缓解后进行的心脏导管检查显示冠状动脉正常。第4天的心脏磁共振成像显示T1和T2值以及细胞外容积分数增加;然而,在她入院当天获取的心肌内膜样本中未观察到炎性细胞的心肌浸润或心肌坏死。怀疑为非典型TTS,给予培哚普利、比索洛尔和螺内酯治疗。TTS发病1.5个月后的磁共振成像显示左心室收缩力、T1和T2值以及细胞外容积分数有所改善。
更详细地了解抗癌药物与TTS之间的关系对于预防抗癌治疗的中断至关重要。