Department of Surgery, Hospital General de Granollers, Granollers, Spain.
School of Medicine, Universitat Internacional de Catalunya, Sant Cugat del Vallès, Barcelona, Spain.
BJS Open. 2024 Jul 2;8(4). doi: 10.1093/bjsopen/zrae080.
There is controversy regarding the maximum number of elements that can be included in a surgical site infection prevention bundle. In addition, it is unclear whether a bundle of this type can be implemented at a multicentre level.
A pragmatic, multicentre cohort study was designed to analyse surgical site infection rates in elective colorectal surgery after the sequential implementation of two preventive bundle protocols. Secondary outcomes were to determine compliance with individual measures and to establish their effectiveness, duration of stay, microbiology and 30-day mortality rate.
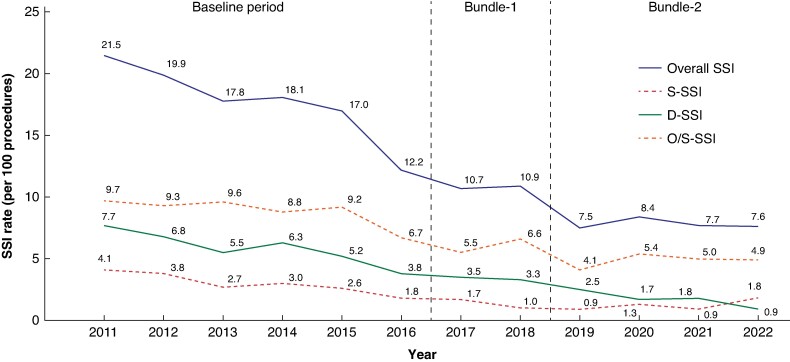
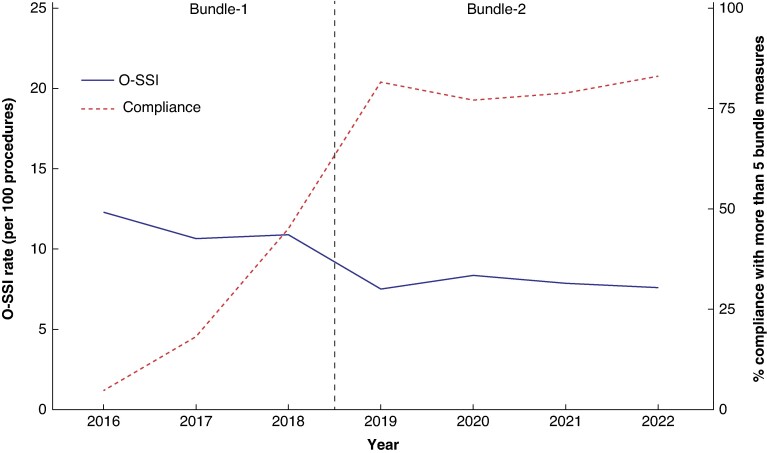
A total of 32 205 patients were included. A 50% reduction in surgical site infection was achieved after the implementation of two sequential sets of bundles: from 18.16% in the Baseline group to 10.03% with Bundle-1 and 8.19% with Bundle-2. Bundle-2 reduced superficial-surgical site infection (OR 0.74 (95% c.i. 0.58 to 0.95); P = 0.018) and deep-surgical site infection (OR 0.66 (95% c.i. 0.46 to 0.93); P = 0.018) but not organ/space-surgical site infection (OR 0.88 (95% c.i. 0.74 to 1.06); P = 0.172). Compliance increased after the addition of four measures to Bundle-2. In the multivariable analysis, for organ/space-surgical site infection, laparoscopy, oral antibiotic prophylaxis and mechanical bowel preparation were protective factors in colonic procedures, while no protective factors were found in rectal surgery. Duration of stay fell significantly over time, from 7 in the Baseline group to 6 and 5 days for Bundle-1 and Bundle-2 respectively (P < 0.001). The mortality rate fell from 1.4% in the Baseline group to 0.59% and 0.6% for Bundle-1 and Bundle-2 respectively (P < 0.001). There was an increase in Gram-positive bacteria and yeast isolation, and reduction in Gram-negative bacteria and anaerobes in organ/space-surgical site infection.
The addition of measures to create a final 10-measure protocol had a cumulative protective effect on reducing surgical site infection. However, organ/space-surgical site infection did not benefit from the addition. No protective measures were found for organ/space-surgical site infection in rectal surgery. Compliance with preventive measures increased from Bundle-1 to Bundle-2.
在外科部位感染预防套件中,可以包含的元素数量存在争议。此外,尚不清楚这种类型的套件是否可以在多中心层面实施。
设计了一项实用的多中心队列研究,以分析择期结直肠手术后,连续实施两套预防套件后的外科部位感染率。次要结果是确定单个措施的依从性并确定其有效性、住院时间、微生物学和 30 天死亡率。
共纳入 32205 例患者。在实施两套连续的套件后,外科部位感染率降低了 50%:从基线组的 18.16%降至套件 1 的 10.03%和套件 2 的 8.19%。套件 2 降低了浅表外科部位感染(OR 0.74(95%置信区间 0.58 至 0.95);P=0.018)和深部外科部位感染(OR 0.66(95%置信区间 0.46 至 0.93);P=0.018),但不包括器官/腔隙外科部位感染(OR 0.88(95%置信区间 0.74 至 1.06);P=0.172)。套件 2 增加了四项措施后,依从性增加。在多变量分析中,对于器官/腔隙外科部位感染,腹腔镜、口服抗生素预防和机械肠道准备是结肠手术的保护因素,而直肠手术中没有发现保护因素。住院时间随着时间的推移显著下降,从基线组的 7 天分别降至套件 1 和套件 2 的 6 天和 5 天(P<0.001)。死亡率从基线组的 1.4%降至套件 1 和套件 2 的 0.59%和 0.6%(P<0.001)。器官/腔隙外科部位感染中,革兰氏阳性菌和酵母的分离增加,革兰氏阴性菌和厌氧菌减少。
增加措施以创建最终的 10 项措施方案对降低外科部位感染具有累积保护作用。然而,器官/腔隙外科部位感染并未从中受益。直肠手术中没有发现器官/腔隙外科部位感染的保护措施。预防措施的依从性从套件 1 增加到套件 2。