Quek Joo Wei Ethan, Loo Jing Hong, Lim En Qi, Chung Ambrose Hon-Lam, Othman Abu Bakar Bin, Tan Jarell Jie-Rae, Barnett Scott, Nguyen Mindie H, Wong Yu Jun
Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
Department of Gastroenterology & Hepatology, Changi General Hospital, Singapore.
EClinicalMedicine. 2024 Jul 13;74:102727. doi: 10.1016/j.eclinm.2024.102727. eCollection 2024 Aug.
Pregnant women with hepatitis C virus (HCV) infection represent a special population in which treatment access remains limited despite its increasing prevalence. A reliable estimate of the burden and clinical outcomes of pregnant women with HCV infection is crucial for HCV elimination. We aimed to determine the prevalence, maternal-to-child transmission (MTCT), maternal and fetal complication rates, and direct acting antivirals (DAA) treatment outcomes of chronic HCV infection in pregnant women.
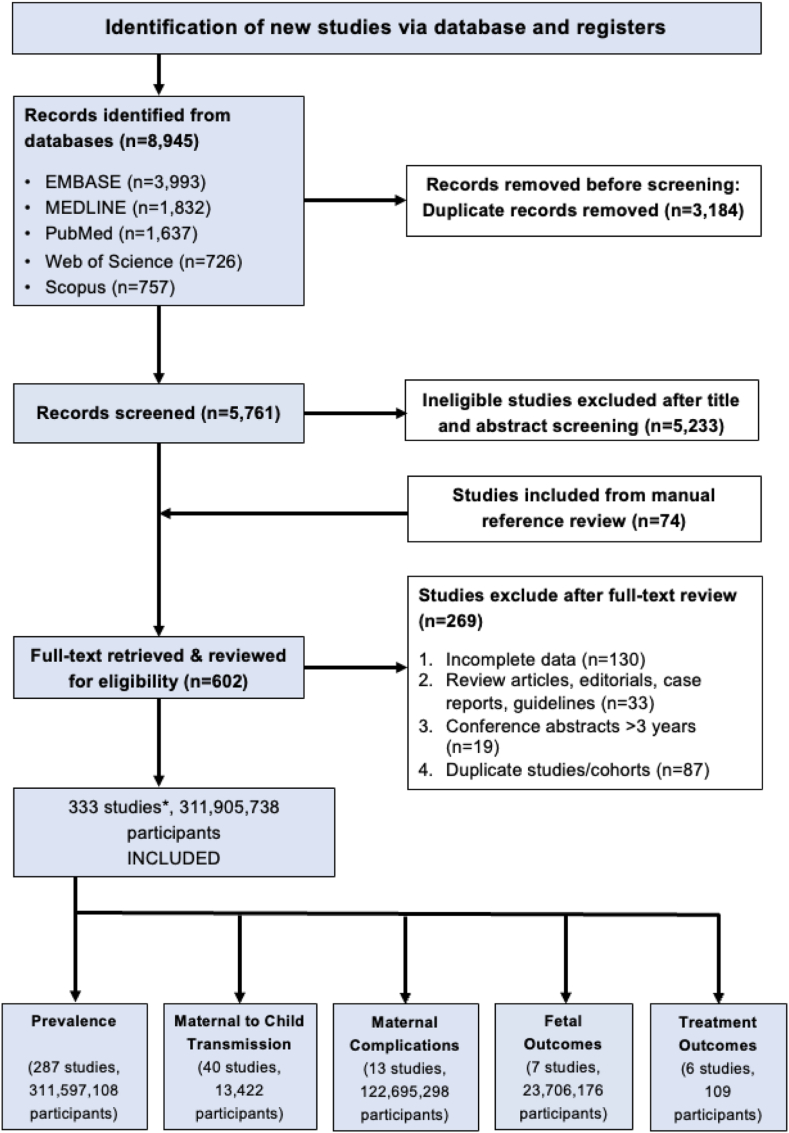
We searched PubMed, EMBASE, Scopus, Web of Science from inception until March 1, 2024, for studies reporting on the prevalence, MTCT, complications of HCV infection, and treatment outcomes of DAA in pregnant women. Study quality was assessed using the Newcastle-Ottawa Scale. We performed subgroup analysis based on 9 variables to explore the source of heterogeneity in HCV prevalence. The PROSPERO registration number is CRD42024500023.
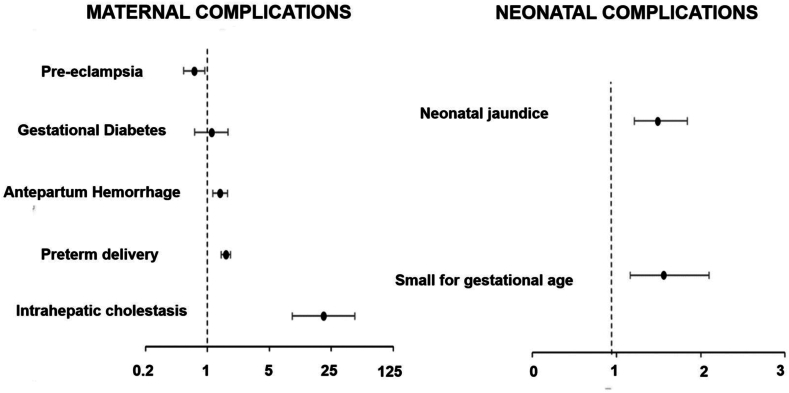
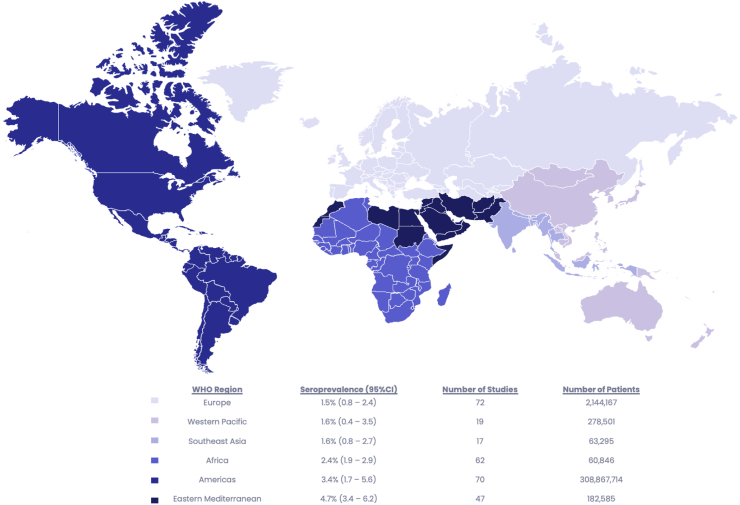
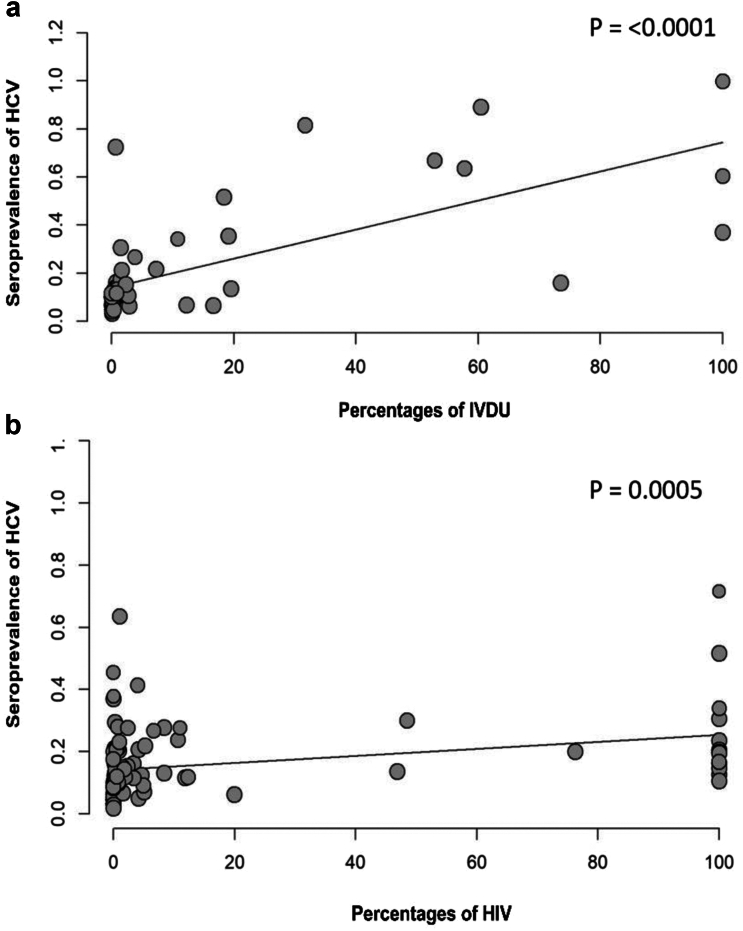
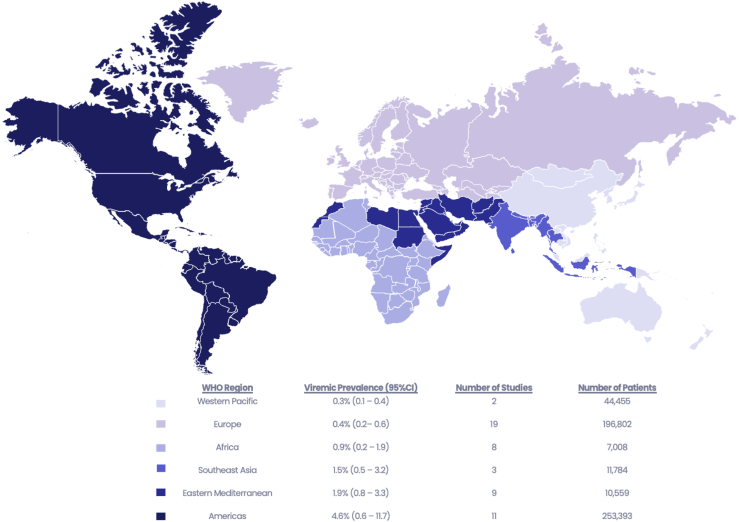
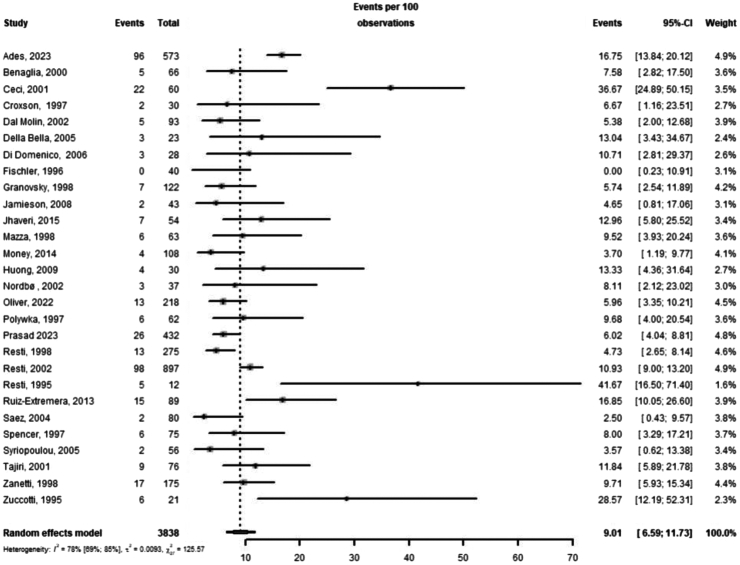
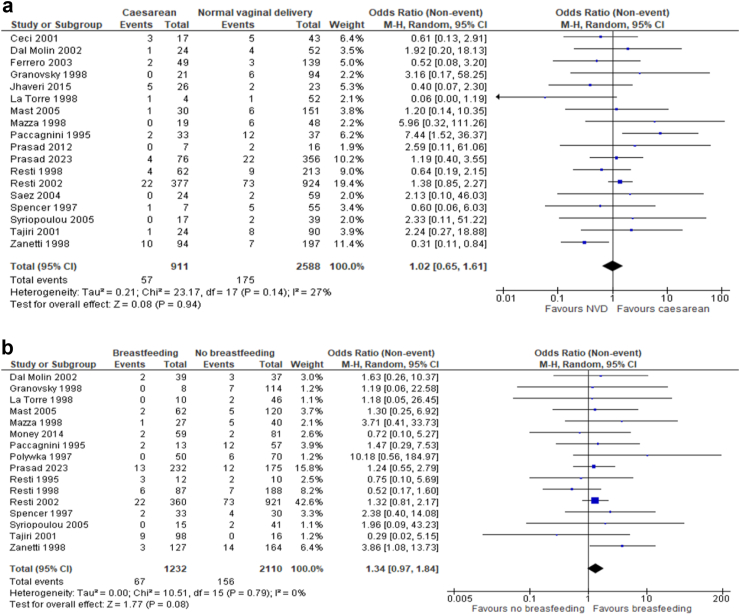
From a total of 311,905,738 pregnant women from 333 studies, the pooled global seroprevalence of HCV in pregnant women was 2.6% (95% CI: 2.0-3.2, = 100%) which increased in patients with intravenous drug use and HIV. Majority of the HCV cases in pregnant women (75%) are diagnosed through universal screening. The pooled MTCT rate was 9.0% (95% CI: 6.6-11.7, = 79%), which was higher with HIV co-infection (OR: 3.1, 95% CI: 2.1-4.6, = 10%), but was not influenced by the mode of delivery or breastfeeding. Pregnant women with HCV infection had more maternal complications, including intrahepatic cholestasis, preterm delivery, and antepartum hemorrhage. Neonates of mothers with HCV had higher odds of being small for gestational age. The pooled rate of sustained virologic response (SVR12) among the 74 women treated with DAA during pregnancy was 98.4%, with no serious adverse events reported.
HCV prevalence in pregnant women varies by geographic region and patient population, while MTCT occurs in almost one in ten viremic mothers. The incidence of both maternal and neonatal complications is significantly higher in patients with HCV infection. Limited data suggest that DAA are safe in pregnant women with HCV infection.
None.
丙型肝炎病毒(HCV)感染的孕妇是一个特殊群体,尽管其患病率不断上升,但获得治疗的机会仍然有限。可靠估计HCV感染孕妇的负担和临床结局对于消除HCV至关重要。我们旨在确定孕妇慢性HCV感染的患病率、母婴传播(MTCT)、母婴并发症发生率以及直接抗病毒药物(DAA)的治疗效果。
我们检索了从创刊至2024年3月1日的PubMed、EMBASE、Scopus、Web of Science数据库,以查找关于孕妇HCV感染的患病率、MTCT、并发症以及DAA治疗效果的研究报告。使用纽卡斯尔-渥太华量表评估研究质量。我们基于9个变量进行亚组分析,以探讨HCV患病率异质性的来源。PROSPERO注册号为CRD42024500023。
在来自333项研究的总共311,905,738名孕妇中,全球孕妇HCV血清学合并患病率为2.6%(95%置信区间:2.0 - 3.2,I² = 100%),在静脉吸毒者和HIV患者中患病率有所增加。孕妇中大多数HCV病例(75%)通过普遍筛查确诊。合并MTCT率为9.0%(95%置信区间:6.6 - 11.7,I² = 79%),HIV合并感染时该率更高(比值比:3.1,95%置信区间:2.1 - 4.6,I² = 10%),但不受分娩方式或母乳喂养的影响。HCV感染孕妇有更多的母体并发症,包括肝内胆汁淤积、早产和产前出血。HCV感染母亲的新生儿小于胎龄的几率更高。在孕期接受DAA治疗的74名女性中,持续病毒学应答(SVR12)合并率为98.4%,未报告严重不良事件。
孕妇HCV患病率因地理区域和患者群体而异,而MTCT发生在几乎每十名病毒血症母亲中就有一名。HCV感染患者的母婴并发症发生率均显著更高。有限的数据表明,DAA对HCV感染孕妇是安全的。
无。