Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241271946. doi: 10.1177/15330338241271946.
To improve the setup reproducibility of neck curvature using real-time optical surface imaging (OSI) guidance on 2 regions of interest (ROIs) to infer cervical spine (c-spine) curvature for surface-guided radiotherapy (SGRT) of head-and-neck (HN) and c-spine cancer.
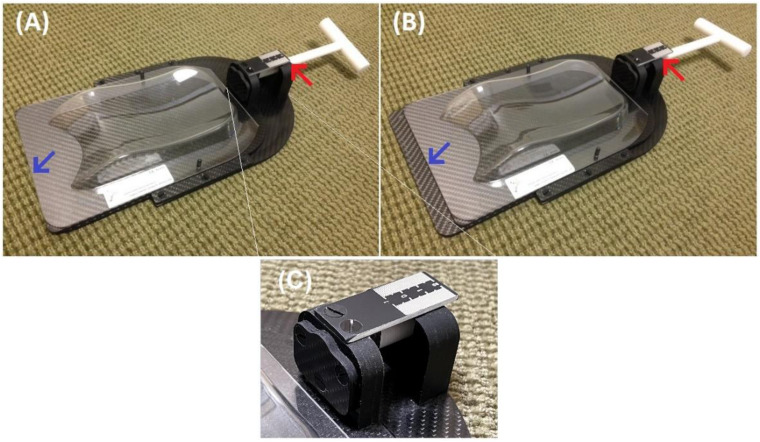
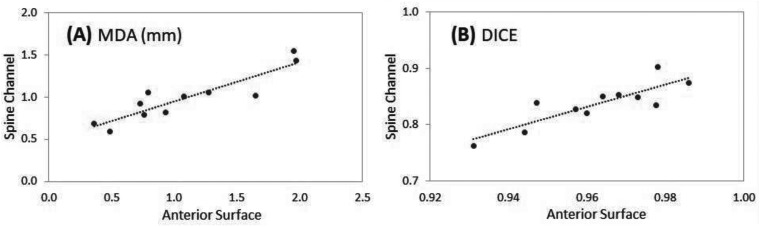
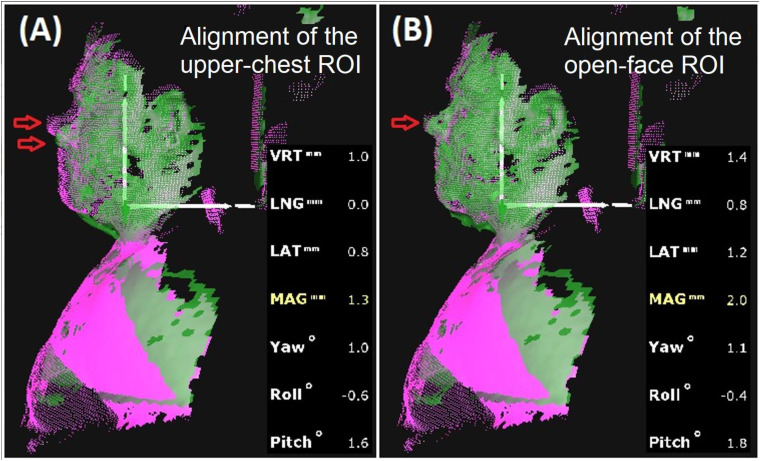
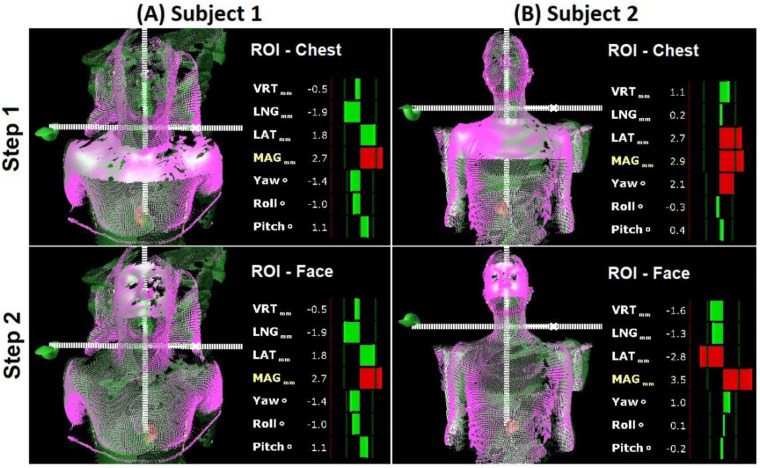
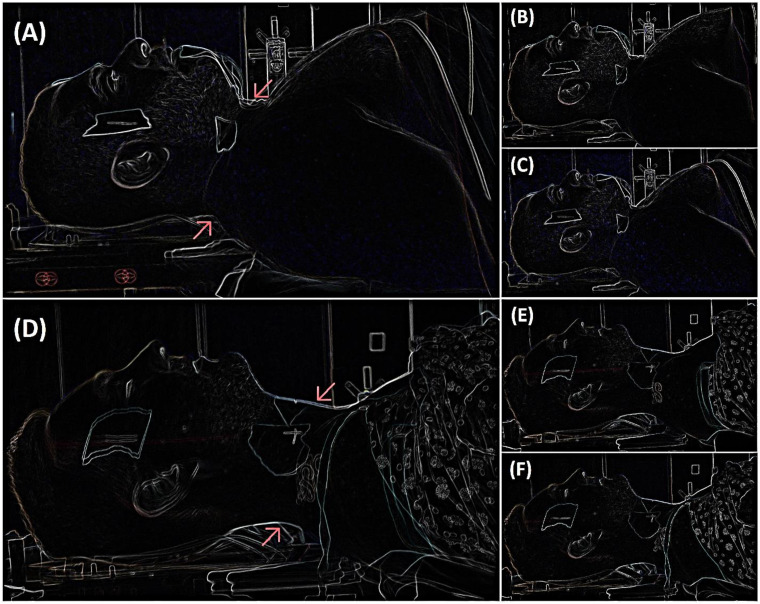
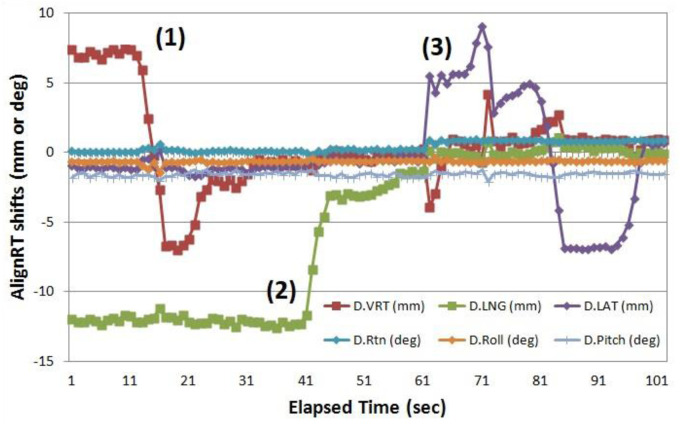
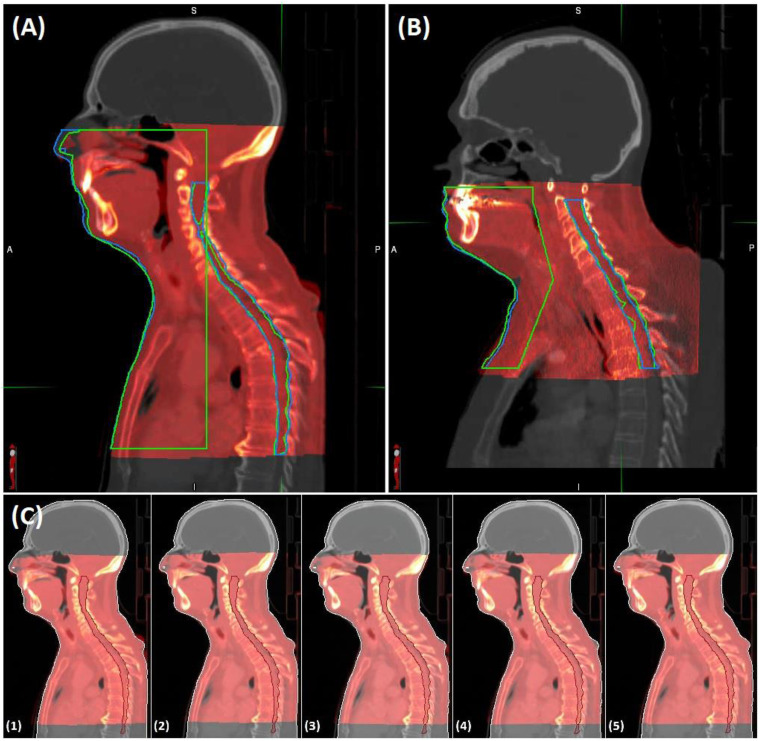
A novel SGRT setup approach was designed to reproduce neck curvature with 2 ROIs: upper-chest ROI and open-face ROI. It was hypothesized that the neck curvature could be reproduced if both ROIs were aligned within ±3 mm/2˚ tolerance. This was tested prospectively in 7 volunteers using real-time 3D-OSI guidance and lateral 2D-photography verification after the 3D and 2D references were captured from the initial conventional setup. Real-time SGRT was performed to align chest-ROI and face-ROI, and the longitudinal distance between them was adjustable using a head-support slider. Verification of neck curvature anteriorly and posteriorly was achieved by overlaying edge-extracted lateral pictures. Retrospectively, the relationship between anterior surface and spinal canal alignment was checked in 11 patients using their simulation CT (simCT) and setup cone-beam CT (CBCT). After the anterior surface was rigidly aligned, the spinal canal alignment was checked and quantified using the mean-distance-to-agreement (MDA) and DICE similarity index, and surface-to-spine correlation was calculated.
The reproducibility of neck curvatures using the 2xROI SGRT setup is verified and the mean neck-outline-matching difference is within ±2 mm in lateral photographic overlays. The chest-ROI alignment takes 110 ± 58 s and the face-ROI takes 60 ± 35 s. When the anterior body surface is aligned (MDA = 1.1 ± 0.6 mm, DICE = 0.96 ± 0.02,) the internal spinal canal is also aligned (MDA = 1.0 ± 0.3 mm, DICE = 0.84 ± 0.04) in 11 patients. The surface-to-spine correlation is c = 0.90 (MDA) and c = 0.85 (DICE).
This study demonstrates the feasibility of the novel 2-ROI SGRT setup technique to achieve reproducible neck and c-spine curvature regardless of neck visibility and availability as ROI. Staff training is needed to adopt this unconventional SGRT technique to improve patient setup.
为了提高颈部曲度的设置可重复性,我们使用实时光学表面成像(OSI)对 2 个感兴趣区域(ROI)进行引导,以推断颈椎(c-spine)曲率,从而对头颈部(HN)和 c-spine 癌症进行表面引导放射治疗(SGRT)。
设计了一种新的 SGRT 设置方法,通过 2 个 ROI 来复制颈部曲率:上胸部 ROI 和敞面 ROI。假设如果两个 ROI 都在±3mm/2°的容差范围内对齐,则可以复制颈部曲率。这在 7 名志愿者中进行了前瞻性研究,使用实时 3D-OSI 引导和侧向 2D-摄影验证,在从初始常规设置捕获 3D 和 2D 参考后进行。通过对齐胸部 ROI 和面部 ROI 来进行实时 SGRT,并使用头架滑块调整它们之间的纵向距离。通过叠加提取的侧面图像来验证颈部前后曲率。回顾性地,在 11 名患者的模拟 CT(simCT)和设置锥形束 CT(CBCT)上检查了前表面与椎管对齐的关系。在前表面被刚性对齐后,使用平均一致性距离(MDA)和 DICE 相似性指数检查和量化椎管对齐,并计算表面与脊柱的相关性。
验证了使用 2xROI SGRT 设置复制颈部曲率的可重复性,在侧面摄影叠加中,颈部轮廓匹配的平均差异在±2mm 以内。胸部 ROI 对齐需要 110±58s,面部 ROI 对齐需要 60±35s。当对齐前体表面(MDA=1.1±0.6mm,DICE=0.96±0.02)时,在 11 名患者中,内部椎管也对齐(MDA=1.0±0.3mm,DICE=0.84±0.04)。表面与脊柱的相关性为 c=0.90(MDA)和 c=0.85(DICE)。
本研究表明,无论颈部可见性和 ROI 可用性如何,使用新型 2-ROI SGRT 设置技术都可以实现可重复的颈部和 c-spine 曲率。需要对员工进行培训,以采用这种非传统的 SGRT 技术来提高患者的设置。