Xu Fei, Zhang Cheng
Department of Anesthesiology, School of Medicine, Chengdu Women's and Children's Central Hospital, University of Electronic Science and Technology of China, Chengdu, 610091, China.
Department of Anesthesiology, Cheng Du Xin Jin District Maternal and Child Health Care Hospital, Chengdu, China.
Diabetol Metab Syndr. 2024 Aug 7;16(1):190. doi: 10.1186/s13098-024-01428-3.
Heart failure is a disease that threatens global public safety. In recent years, the obesity paradox has been studied in cardiovascular disease and other fields. With the progress of aging, metabolic changes and regulation of fat function, it also provides many bridges for the dialogue between disease and molecular metabolism. The purpose of this study is to investigate the effect of obesity on the outcome of adult intensive care patients with heart failure combined with age factors.
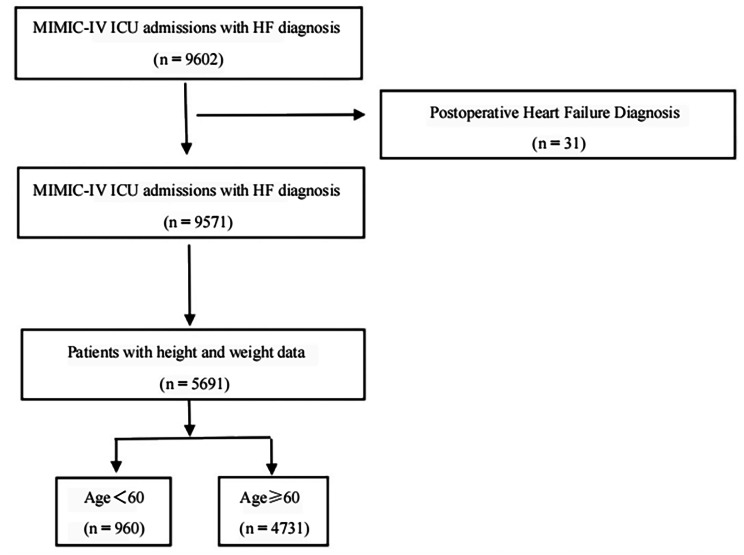
Data were derived from the fourth-generation Medical Information Marketplace for Intensive Care (MIMIC-IV version2.1) using structured query language on the Navicat (12.0.11) platform. People were divided into two groups based on the body mass index (BMI), one group with BMI ≥ 30 kg/m² and another group with BMI < 30 kg/m². Afterwards, the patients were divided into two subgroups based on their ages. One group included patients aged<60, and the other included patients aged ≥ 60. The extracted information includes demographic characteristics, laboratory findings, comorbidities, scores. Main results included in-hospital mortality, ICU mortality, and 1-year mortality. Secondary outcomes included hospital interval and ICU interval, use of renal replacement therapy, and rates of noninvasive and invasive ventilation support.
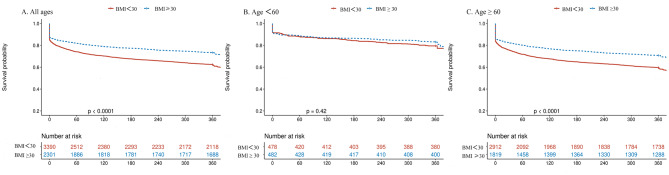
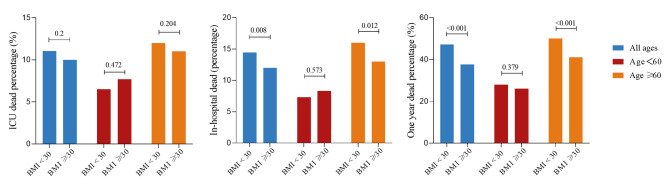
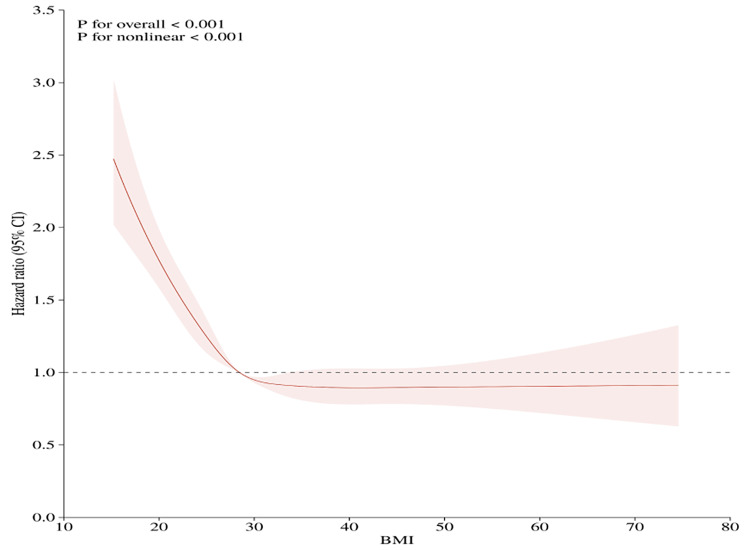
In this cohort study, 3390 people were in the BMI<30 group, 2301 people were in the BMI ≥ 30 group, 960 people were in the age<60 group, and 4731 people were in the age ≥ 60 group, including 3557 patients after propensity score matching in high age group. Among patients aged ≥ 60, BMI ≥ 30 group vs. BMI<30 group showed significantly lower in-hospital mortality (13% vs. 16%) and one-year mortality (41% vs. 55%), respectively. Neither primary nor secondary outcomes were significantly described in the competition among patients aged under 60. Restricted cubic spline reveals a J-shaped nonlinear association between BMI and clinical endpoints within the entire cohort. Kaplan-Meier curves revealed a survival advantage in BMI ≥ 30 group (p < 0.001). Following age stratification, a beneficial effect of BMI categories on one-year mortality risk was observed in heart failure patients aged ≥ 60 (Univariable HR, 0.71, 95% CI, 0.65-0.78, p < 0.001; Multivariable HR, 0.74, 95% CI, 0.67-0.81, p < 0.001), but not in those under 60 years old.
In ICU patients with heart failure, obesity offers a survival benefit to those aged ≥ 60. No obesity paradox was observed in patients younger than 60 years old. The obesity paradox applies to patients aged ≥ 60 with heart failure.
心力衰竭是一种威胁全球公共安全的疾病。近年来,肥胖悖论已在心血管疾病等领域得到研究。随着衰老进程、代谢变化以及脂肪功能的调节,这也为疾病与分子代谢之间的对话搭建了许多桥梁。本研究的目的是探讨肥胖对合并年龄因素的成年重症监护心力衰竭患者预后的影响。
数据来源于第四代重症监护医学信息市场(MIMIC-IV版本2.1),使用Navicat(12.0.11)平台上的结构化查询语言。根据体重指数(BMI)将人群分为两组,一组BMI≥30kg/m²,另一组BMI<30kg/m²。之后,根据年龄将患者分为两个亚组。一组包括年龄<60岁的患者,另一组包括年龄≥60岁的患者。提取的信息包括人口统计学特征、实验室检查结果、合并症、评分。主要结果包括住院死亡率、重症监护病房死亡率和1年死亡率。次要结果包括住院时间和重症监护病房停留时间、肾脏替代治疗的使用情况以及无创和有创通气支持率。
在这项队列研究中,BMI<30组有3390人,BMI≥30组有2301人,年龄<60岁组有960人,年龄≥60岁组有4731人,其中高龄组倾向得分匹配后有3557例患者。在年龄≥60岁的患者中,BMI≥30组与BMI<30组相比,住院死亡率(分别为13%和16%)和1年死亡率(分别为41%和55%)显著降低。在60岁以下患者的比较中,主要和次要结果均无显著差异。限制立方样条显示整个队列中BMI与临床终点之间呈J形非线性关联。Kaplan-Meier曲线显示BMI≥30组具有生存优势(p<0.001)。按年龄分层后,观察到BMI类别对年龄≥60岁的心力衰竭患者1年死亡风险有有益影响(单变量HR,0.71,95%CI,0.65-0.78,p<0.001;多变量HR,0.74,95%CI,0.67-0.81,p<0.001),但在60岁以下患者中未观察到。
在重症监护心力衰竭患者中,肥胖对年龄≥60岁的患者具有生存益处。60岁以下患者未观察到肥胖悖论。肥胖悖论适用于年龄≥60岁的心力衰竭患者。