Janssen Jorien B E, Brahm Cyrillo G, Driessen Chantal M L, Nuver Janine, Labots Mariette, Kouwenhoven Mathilde C M, Sanchez Aliaga Esther, Enting Roelien H, de Groot Jan Cees, Walenkamp Annemiek M E, van Linde Myra E, Verheul Henk M W
Department of Medical Oncology, Research Institute for Medical Innovation, Radboud University Medical Center, 6525 GA, Nijmegen, The Netherlands.
Department of Medical Oncology, Cancer Center Amsterdam, Vrije Universiteit Amsterdam, Amsterdam UMC, 1081 HV, Amsterdam, The Netherlands.
Brain Commun. 2024 Jul 30;6(4):fcae241. doi: 10.1093/braincomms/fcae241. eCollection 2024.
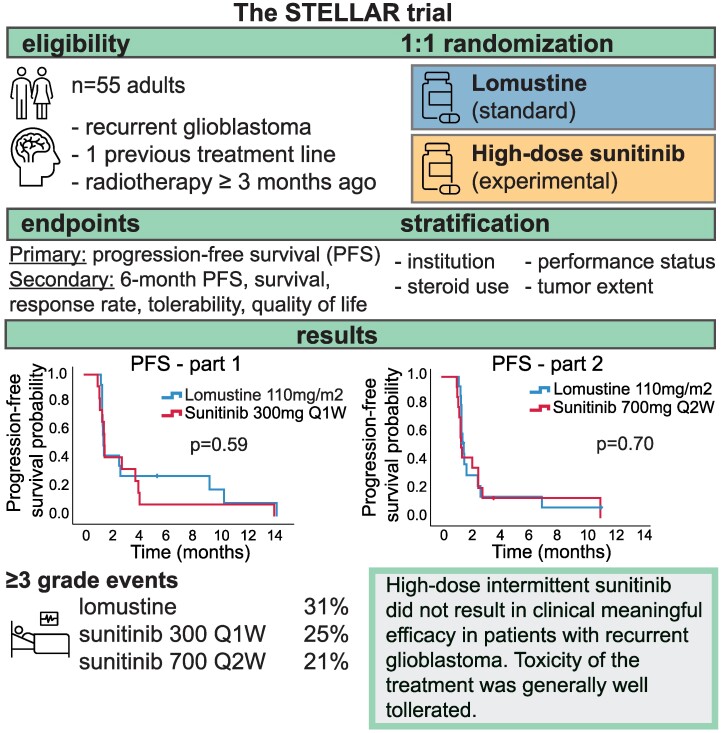
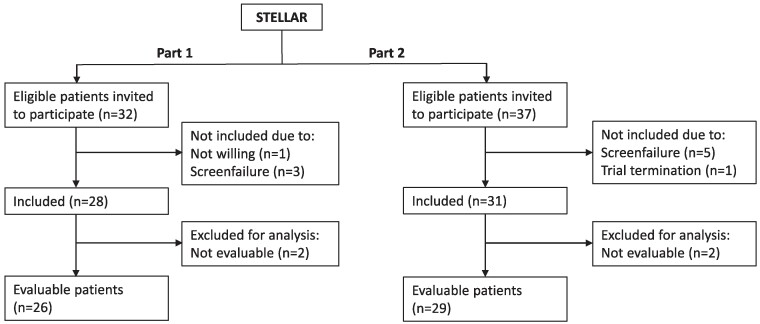
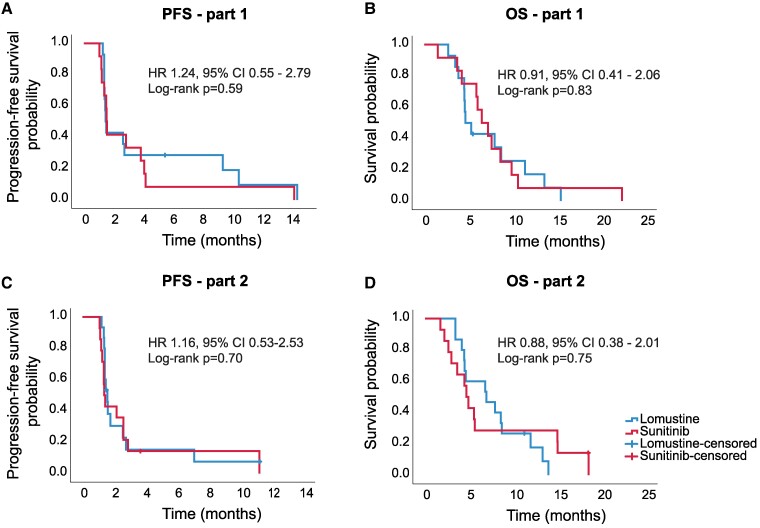
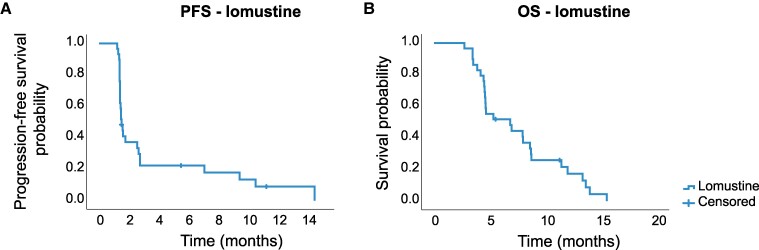
Previously, the tyrosine kinase inhibitor sunitinib failed to show clinical benefit in patients with recurrent glioblastoma. Low intratumoural sunitinib accumulation in glioblastoma patients was reported as a possible explanation for the lack of therapeutic benefit. We designed a randomized phase II/III trial to evaluate whether a high-dose intermittent sunitinib schedule, aimed to increase intratumoural drug concentrations, would result in improved clinical benefit compared to standard treatment with lomustine. Patients with recurrent glioblastoma were randomized 1:1 to high-dose intermittent sunitinib 300 mg once weekly (Q1W, part 1) or 700 mg once every two weeks (Q2W, part 2) or lomustine. The primary end-point was progression-free survival. Based on the pre-planned interim analysis, the trial was terminated for futility after including 26 and 29 patients in parts 1 and 2. Median progression-free survival of sunitinib 300 mg Q1W was 1.5 months (95% CI 1.4-1.7) compared to 1.5 months (95% CI 1.4-1.6) in the lomustine arm ( = 0.59). Median progression-free survival of sunitinib 700 mg Q2W was 1.4 months (95% CI 1.2-1.6) versus 1.6 months (95% CI 1.3-1.8) for lomustine ( = 0.70). Adverse events (≥grade 3) were observed in 25%, 21% and 31% of patients treated with sunitinib 300 mg Q1W, sunitinib 700 mg Q2W and lomustine, respectively ( = 0.92). To conclude, high-dose intermittent sunitinib treatment failed to improve the outcome of patients with recurrent glioblastoma when compared to standard lomustine therapy. Since lomustine remains a poor standard treatment strategy for glioblastoma, innovative treatment strategies are urgently needed.
此前,酪氨酸激酶抑制剂舒尼替尼在复发性胶质母细胞瘤患者中未显示出临床获益。有报道称,胶质母细胞瘤患者肿瘤内舒尼替尼蓄积量低可能是缺乏治疗获益的一个原因。我们设计了一项随机II/III期试验,以评估旨在提高肿瘤内药物浓度的高剂量间歇性舒尼替尼方案与洛莫司汀标准治疗相比是否能带来更好的临床获益。复发性胶质母细胞瘤患者按1:1随机分组,分别接受高剂量间歇性舒尼替尼治疗,即300 mg每周一次(Q1W,第1部分)或700 mg每两周一次(Q2W,第2部分),或洛莫司汀治疗。主要终点是无进展生存期。根据预先计划的中期分析,在第1部分和第2部分分别纳入26例和29例患者后,该试验因无效而终止。舒尼替尼300 mg Q1W组的中位无进展生存期为1.5个月(95%CI 1.4 - 1.